Great Toe Transplantation
Anatomic considerations
Great toe transplantation has proven itself to be the ideal form of thumb reconstruction in cases of traumatic thumb loss and in selected cases of congenital absence of the thumb. The procedure is, however, extremely technically demanding, requiring the utmost of skill from the microsurgeon and microsurgical team. The harvest of the great toe and the inset on the hand can be both challenging and beset by technical hurdles. Postoperative monitoring in an appropriate microsurgical unit is essential to averting potential thrombosis and treating circulatory complications if they happen. Accurate monitoring and early treatment of complications help to achieve a favorable outcome.
Great toe transplantation has proven itself to be the ideal form of thumb reconstruction in cases of traumatic thumb loss and in selected cases of congenital absence of the thumb. The procedure is, however, extremely technically demanding, requiring the utmost of skill from the microsurgeon and microsurgical team. The harvest of the great toe and the inset on the hand can be both challenging and beset by technical hurdles. Postoperative monitoring in an appropriate microsurgical unit is essential to averting potential thrombosis and treating circulatory complications if they happen. Accurate monitoring and early treatment of complications help to achieve a favorable outcome.
Preoperative Assessment
Any traumatic injury or congenital absence requires a thorough preoperative evaluation by the microsurgeon. The hand is examined to determine the anatomy of the loss, suppleness of joints and soft tissues and the potential requirements for reconstruction. Vascular inflow, innervation, bony structure and the presence of adequate controlling tendons are assessed. The need for any further soft tissue reconstruction is identified, such as a second skin or fasciocutaneous transplant or even a local flap . If a great toe transplant is felt to be the reconstruction of choice, the surgeon must evaluate the lower extremity completely. This includes a history of previous injury or surgery, and a complete skeletal, vascular and sensorimotor examination. Particular attention should be paid to the pedal pulses. If arterial inflow is thought to be questionable whether by history or physical examination, then an angiographic study of the lower extremity is performed. We however do not routinely perform angiography of the lower extremity because we have found the vessel spasm of the foot to be particularly problematic in angiography. This often leads to results that are of no value, i.e. poor visualization of the small vessels in the foot and to the toes. In healthy individuals with no clear indication for angiography, the study does not help the surgeon either plan or perform the surgical procedure.
Anatomy
The great toe has a single interphalangeal joint like the thumb, and in most patients the total length of the great toe is comparable to that of the thumb. However, the transverse diameter and bulk of the toe are comparatively large (many authors believe there is some atrophy after transplantation).
Toe extension is provided by the extensor hallucis longus and brevis tendons. The longus is typically repaired to the extensor pollicis longus of the thumb.
The arterial inflow to the great toe can be from the dorsal or plantar system, depending on the dominance of supply. This varies between patients. The superficial venous system can almost always be used for venous drainage. The long extensor is used for extensor reconstruction.
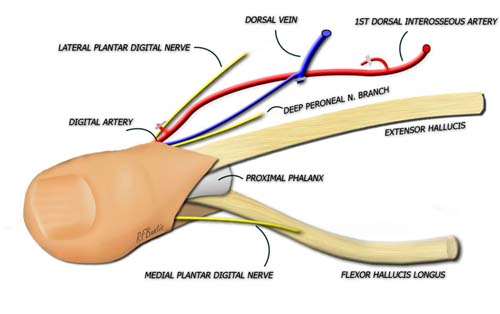
Flexion is provided by the flexor hallicus longus and brevis muscles, with the longus used for thumb reconstruction when attached to the flexor pollicus longus . The plantar digital nerves provide sensation, and travel volar to the deep transverse metatarsal ligament (not shown below). The lateral digital nerve is short and often requires intraneural dissection from the common digital to gain extra length when necessary for the transplant. The flap is typically disarticulated at the metatarsophalangeal joint, but it can also be taken distal to this level. More distally, great caution must be taken not to injure the small digital vessel supplying arterial inflow.
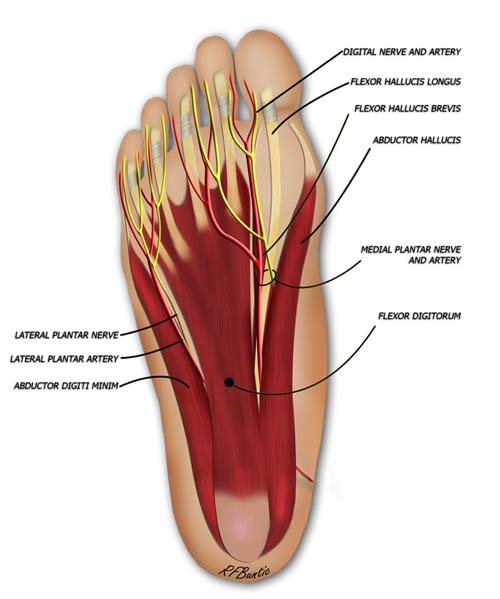
The nerve supply to the flap is from the plantar digital system. The plantar artery runs adjacent to the common digital nerve of the first web space.
Venous Anatomy
The large plexus of veins on the dorsum of the foot can be marked preoperatively with a venous tourniquet about the ankle and the foot placed in a dependent position. The dorsal venous arch has multiple interconnections and drainage via the greater and lesser saphenous systems. This system allows a long pedicle for the venous drainage that can be easily dissected proximally.
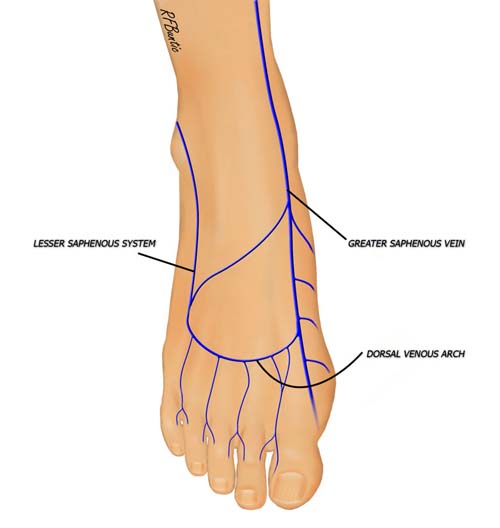
The dorsal venous network supplies an abundance of vascular outflow choices that can be used for venous drainage.
Vascular Anatomy
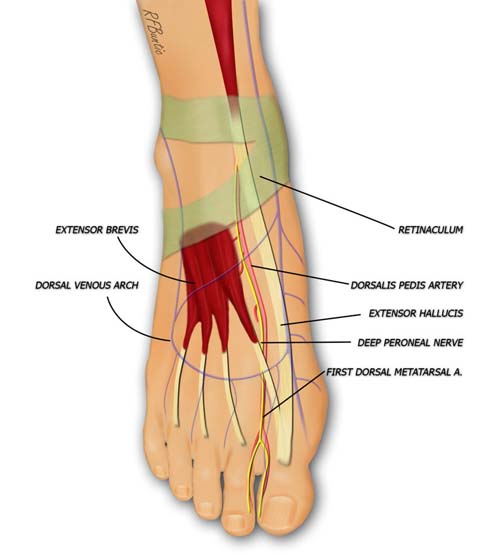
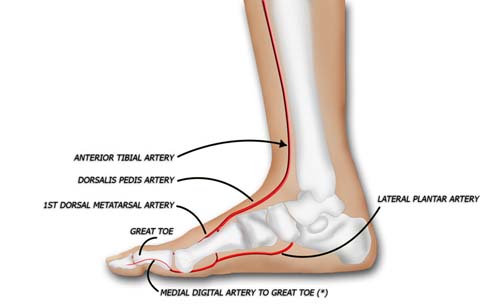
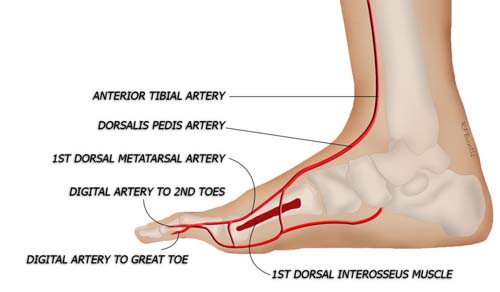
Arterial inflow to the great toe is supplied by both the first dorsal metatarsal artery and the first plantar metatarsal artery, one of which is usually dominant. In our experience, approximately 60% of patients have a plantar dominant system. Occasionally, both dorsal and plantar systems are of similar caliber. A strong Doppler signal extending from the dorsalis pedis to the first web space ordinarily means a good dorsal inflow will be present. Both systems communicate via branches that dive between the metatarsals and send arterial inflow into the toes.
The medial digital artery of the great toe is typically small, and the larger branch in the first web space is used for inflow.
In the figure below, the second metatarsal and second toe are revealed from a medial perspective, after the great toe and first metatarsal have been peeled away. Communicating branches between the dorsal and plantar systems are visible, as are the branches to the second toe, and the transected branches to the great toe. This anatomy can be quite often variable with the first dorsal system diving through or deep to the first dorsal interosseous muscle. The muscle may need to be divided or an intramuscular dissection may need to be performed to expose the dominant inflow system. Our preference is to vein graft rather than to disrupt the entire first interspace.
In this view, the proximal and distal phalanx of the great toe have been removed, to visualize the vascular system in the first web space. The dorsal and plantar systems interconnect in the space between the metatarsals. The dorsal and plantar digital arteries are inspected and the larger of the two is harvested for the flap.
If plantar dominance requires dissection of the vessel proximally on the plantar aspect, the vessel may be traced to the dorsal pedis if the first dorsal interosseous muscle is divided. Some authors recommend vein grafting to the distal plantar dominant system and avoiding the tedious plantar dissection. The disadvantage of vein grafting include a potential increase in the rate of thrombosis and a smaller caliber artery that is present distally.
Dissection
The major draining veins of the great toe are usually drawn on the dorsum of the foot with a marking pen and the incision is outlined as shown below. The incision extends into the first web space and laterally to a level just distal the the metatarsophalangeal joint. Medially, the surgeon should consider a design that leaves sufficient flap length to enable closure of the wound with minimal, if any, shortening of the first metatarsal.

The dorsal incision is placed distal to the metatarsophalangeal joint medially and into the first web space laterally.
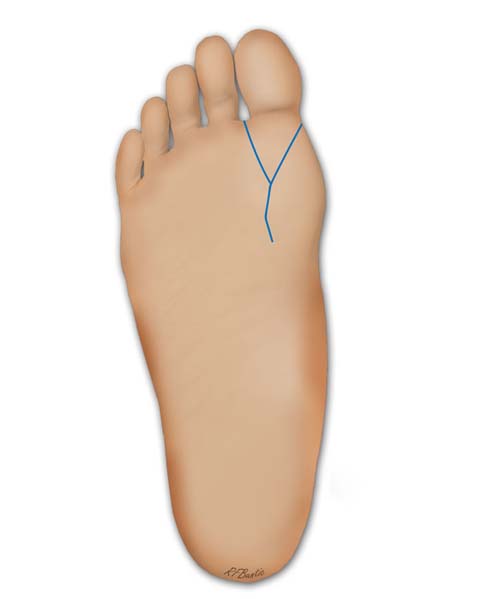
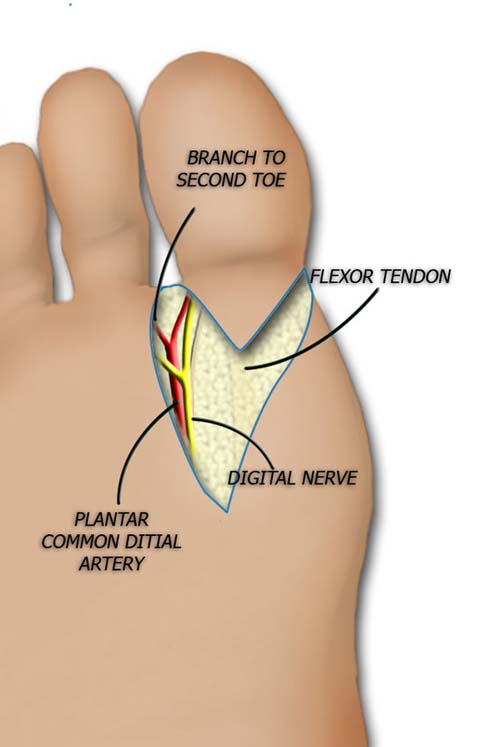
The plantar incision is "v" shaped and extends over the flexor tendon.
Attention is turned first to the first web space where the dissection proceeds to identify the arterial branches to the great and second toes, and then more proximally the dominant arterial supply. If the system is dorsal, the bulk of the rest of the dissection proceeds with relative ease dorsally, isolating the first dorsal metatarsal artery and the great toe extensor and a major draining vein.

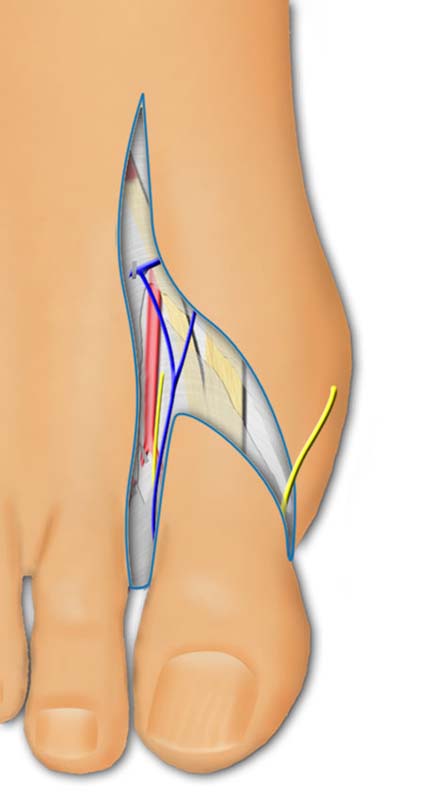
The artery is identified in the first web space and a decision to harvest the plantar or medial arterial system can be made.
If the arterial inflow is plantar dominant, the dorsal dissection can be continued to isolate the extensor tendon and a dorsal vein. The plantar dissection will then not only require the usual exposure of the flexor tendon and nerves, but will also entail dissection of the plantar digital artery to the great and second toes. In the plantar fat this can be tedious, and particularly tedious if the vessel wraps medially around the plantar sesamoid bone of the great toe.
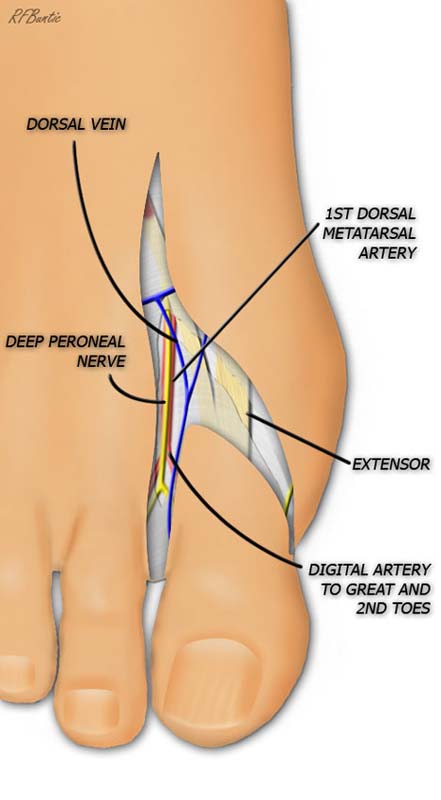
The artery is identified in the first web space. The deep peroneal nerve is used optionally if the recipient hand has a dorsal radial nerve in proximity for repair.
Once the plantar digital nerves and flexor tendon are dissected free and transected, attention can be turned to the joint capsule. The metatarsophalangeal joint is disarticulated while protecting the pedicle and draining vein.
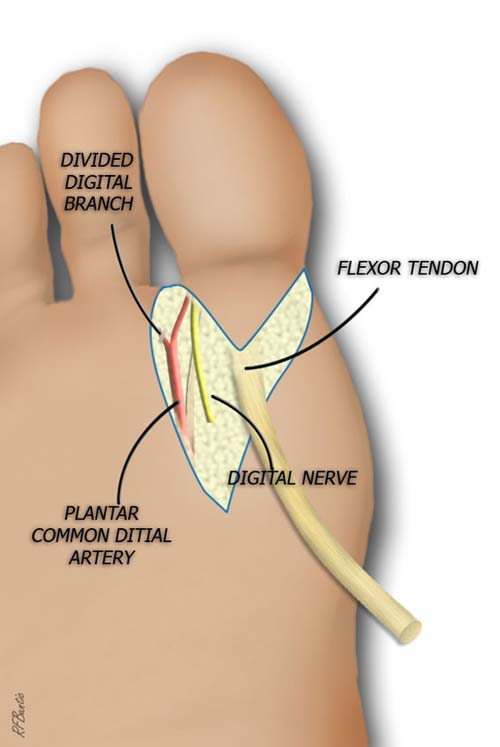
The medial digital plantar nerve is identified, dissected proximally and transected.
The artery is ligated and nerves isolated. The lateral plantar digital nerve can be divided. The nerve to the second toe is spared.
When the recipient team is ready, the dominant artery and vein are ligated and transected.
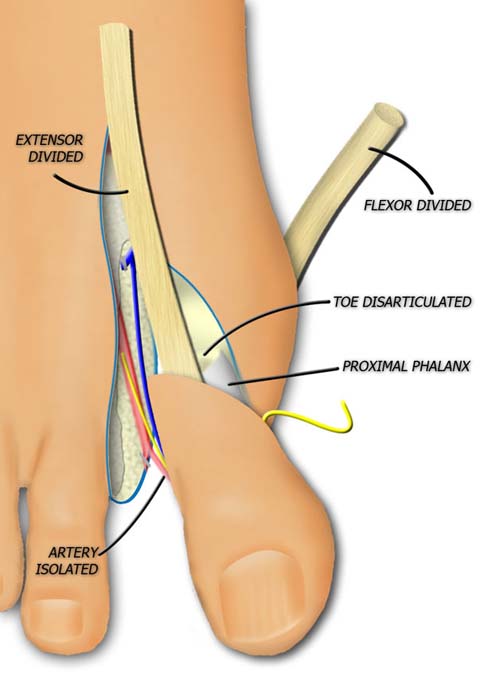
The extensor tendon is divide and the metatarsophalangeal joint is disarticulated.
The flexor tendon is divided and the artery and vein are ligated and divided.
The toe is isolated and ready for transferring to the hand.
The would is closed without tension to avoid necrosis of the medial flap.

The donor area is closed.
Post-Operative Care
The foot is kept elevated for the first week and then introduced to a progressive dangling regimen. An ace wrap can provide gentle compression during dangling. Weight bearing is not begun until the donor site is well healed, often not until four to six weeks. During this time crutch use can be difficult because use of the reconstructed hand is limited. In bilateral toe transplants crutches are not used. In these cases special shoes that keep the feet in exaggerated dorsiflexion can be used to limit plantar weight and transfer weight to the heels.
Significant wound complications are rare in the healthy patient. If a vascular complication in the transplanted toe requires systemic patient heparinization, then hemorrhage into donor site can cause ecchymosis, flap necrosis and delayed healing. This is treated according to the severity of any wound development. Rehabilitation with dangling and subsequent ambulation are delayed.