Latissimus Dorsi Muscle Flap
Anatomic considerations
The latissimus dorsi muscle is the largest muscle in the body, up to 20 by 40 centimeters, allowing coverage of extremely large wounds. In spite of its size, no significant donor functional deficit results from removal of the muscle. It is the largest flap that can be harvested on a single predicle, and can even be combined with the serratus, scapular or parascapular flaps, to create a flap complex that can cover massive wounds. In the normal population the muscle is quite thin (less than 1 centimeter thick), allowing it to be draped over irregular surfaces with ease. With the rectus muscle and radial forearm flap, it represents one of the workhorse flaps in reconstructive microsurgery. When re-innervated using the thoracodorsal nerve, the latissimus can be used as a functional muscle.
Anatomy
The muscle takes origin on the iliac crest inferiorly and the thoracolumbar fascia posteriorly near the midline. It inserts into the humerus where it acts as a humeral adductor and internal rotator. The posterior axillary fold is made up of the most superior aspect of the muscle that begins to narrow before it forms the tendon of insertion. The nerve supply is via the thoracodorsal nerve, a branch of the posterior cord of the brachial plexus. Lesions of C-7 will affect latissimus function. The nerve closely accompanies the thoracodorsal artery.
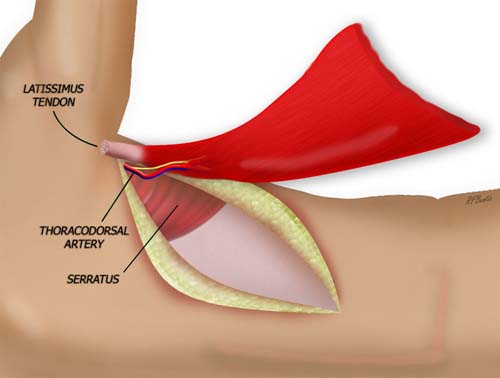
Anatomy Figure 1
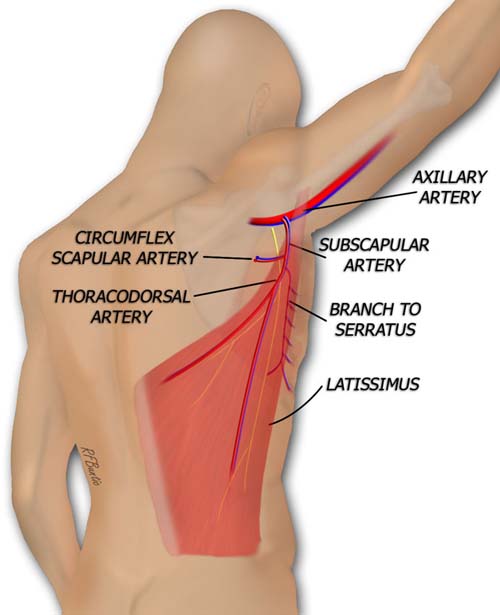
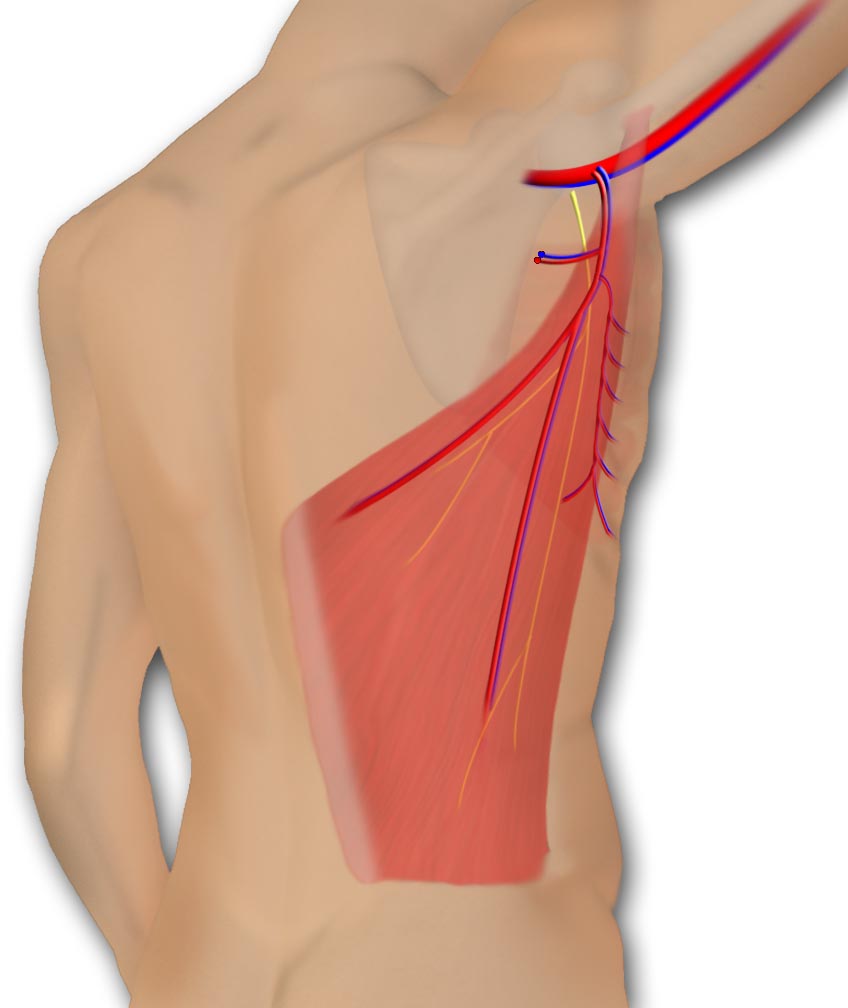
The latissimus muscle is supplied by the thoracodorsal artery, and branch of the subscapular artery. A nerve, the thoracodorsal, and vein accompany the artery.
The latissimus muscle blood supply is via the subscapular artery, a branch of the axillary artery.
The subscapular sends off a circumflex scapular branch posteriorly and then distributes a serratus branch before it enters the substance of the muscle on its undersurface.
On the subscapular system a 5 to 15 centimeter pedicle can be obtained. There is typically a single venae commitans accompanying the artery. The pedicle can be approached directly by dissecting the latissimus from the axilla, or it can be found by following the undersurface of the muscle in a distal to proximal approach. Because the artery divides in the substance of the muscle, the muscle can be split longitudinally to to form a bilobed or two tongued flap. The superior portion of the muscle can be taken on a transverse intramuscular branch of the thoracodorsal vessels: this flap is called the partial superior latissimus flap.
The subscapular artery can be from 2 to 5 millimeters in size, while the thoracodorsal artery ranges from 1 to 3 millimeters. The venae commitans is usually slightly larger.
The muscle is also supplied by perforators from the thoracic intercostal and lumbar arteries that allow it to be used as a pedicled flap that can resurface posterior defects. These vessels are quite small with short leashes and not typically used for microsurgical reconstruction.
Operative Procedure
The patient is placed in the lateral decubitus position on a beanbag, with an axillary roll placed in the dependent axilla. The ipsilateral arm is prepped completely and left in the operative field, allowing it to be freely moved about the field. For most of the procedure it is kept abducted and resting on a well padded sterile Mayo stand placed anterosuperiorly to the patient. The latissimus border is outlined with a marking pen. The incision is then marked extending from the axilla or the posterior axillary fold, then inferiorly and medially over the latissimus muscle. The length of muscle needed will dictate the incision length. Alternatively, if a skin paddle is necessary, it is marked over the flap. A pencil Doppler can be used to ensure the presence of a perforator in the skin paddle.
Operative Procedure: Figure 1
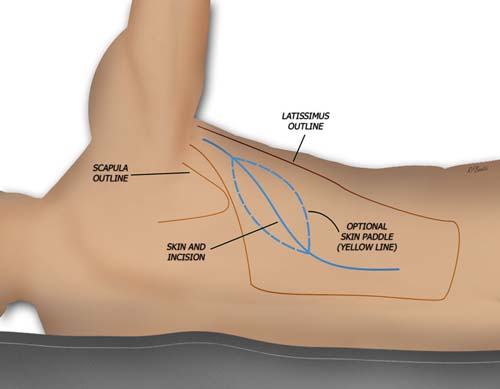
The patient is marked in the lateral decubitus position for the extent of the muscle, skin incision and possible skin paddle.
Anterior and posterior flaps are raised superficial to the muscle to expose the latissimus. A small amount of muscular fascia can be left on the latissimus, but this is not necessary. Any comfortable plane for the surgeon is adequate. The skin and fat flaps are elevated to the extent of the pocket necessary for adequate muscle size harvest. Smaller muscle can be taken if the entirety of the muscle is not needed.
The superior edge of the latissimus is identified at the inferior angle of the scapula. The serratus muscle can be identified easily with this approach. The alternate approach from distal to proximal can often lead to confusion and unnecessary elevation of the serratus muscle since the distal serratus latissimus plane is less apparent.. When elevating the flap from inferior to superior it is important not to dissect underneath the serratus.
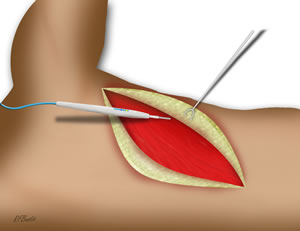
The pocket is dissected
The superior edge of the latissimus, below the inferior angle of the scapula is then elevated. This areolar plane is easy to dissect, and any large caliber perforators can be ligated and divided. The dissection is then directed toward the midline, and the insertions of the muscle near the midline of the back is divided. The dissection proceeds inferiorly freeing the medial muscle insertion.
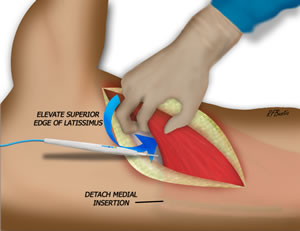
The superior edge of the muscle is elevated
When the inferior portion of the muscle is reached, the attachment plane here is not clear and muscle be created with the electrocautery. After the medial and inferior muscle is released, the dissection proceed underneath the muscle toward the axilla. The plane becomes very thin and areolar and easy to dissect.
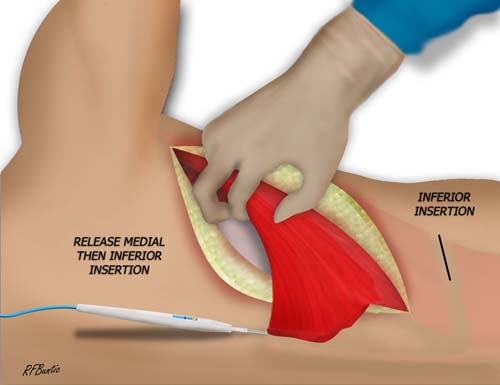
The muscle is freed of medial and inferior attachments
The vessels to the latissimus and serratus become clear as the axilla is neared. The branch to serratus is ligated and the circumflex scapular branch can be if more length is needed. The nerve is divided and the artery and vein can be ligated and divided when the recipient area is ready.
The muscle harvest is complete and pedicle remains attached
The wound is closed with a deep and superficial layer. Two suction drains are place through the anterior skin flap.
Postoperative Care
We allow the patient to use the ipsilateral arm postoperatively and no special dressings are required. The donor area should be inspected daily for hematoma formation. This donor area often forms a seroma, necessitating the use of drains for often more than a week. We often leave them in for 2 weeks or longer until the output is diminished. Seromas should be aspirated.