The Medial Plantar Flap
Anatomic considerations
Anatomy
The skin and fascia over the medial aspect of the foot is thin, providing glabrous tissue for reconstruction of a variety of small soft tissue defects. The skin is supplied by perforators from the medial plantar branch of the posterior tibial artery. The venous system is quite thin and small, and the subcutaneous system is easily incorporated into the flap and used for venous drainage. The flap length varies by defect size, with the width allowing primary closure at most 2 centimeters. If a wider flap is necessary, the defect must be skin grafted.
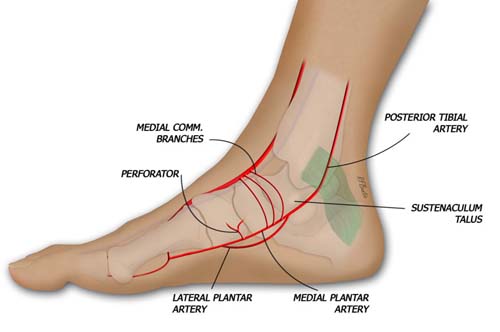
The medial plantar flap is supplied by a perforating system fro the medial plantar artery, a branch of the posterior tibial artery.
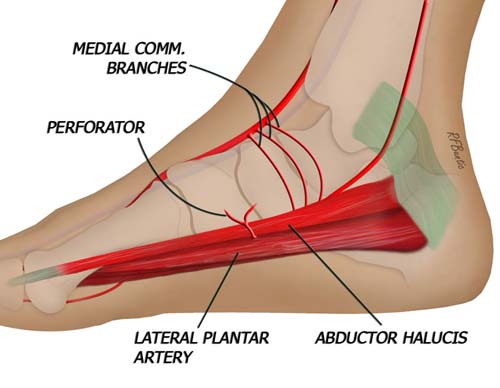
The perforator exits between the abductor hallucis and flexor brevis muscles.
Operative Procedure
The patient is prepped and draped supine, and a well padded thigh tourniquet is used for the procedure once the flap anatomy is defined. The flap is marked on an axis between the sustentaculum of the talus and the medial aspect of the head of the first metatarsal. The perforator from the medial plantar artery arises approximately a third of the way between the sustentaculum and the metatarsophalangeal joint. The location of the perforator is confirmed with a pencil Doppler.

The perforator to the flap can be identified with a Doppler pencil, and the flap can be designed to incorporate the perforator to the flap.
The flap is raised starting at the plantar aspect first, dissecting toward the dorsal aspect of the foot while deep to the muscular fascia over the flexor hallucis brevis muscle. As one dissects towards the dorsum of the foot, the perforator is encountered between the heads of the flexor hallucis brevis and abductor hallucis muscles. We have found the abductor hallucis to be quite small on occasion, without a muscular presence at this level. The perforator then appears to lie on the bone surface.
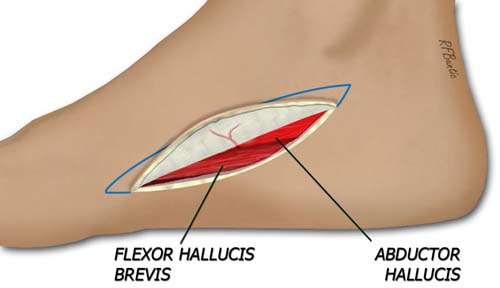
The flap is elevated starting at the plantar aspect, deep to the muscular fascia. The perforator is identified between the flexor and abductor hallucis muscles.
The perforator is then dissected toward its origin on the medial plantar artery in the intermuscular space. A pedicle length of up to 3 centimeters can be made. When the anterior surface of the flap is elevated, the superficial venous system is spared and a subcutaneous vein is followed toward the saphenous system to allow for a larger draining vein for this flap. The vein on the medial plantar system can be quite small.
If desired, a cutaneous nerve branch from the posterior tibial system can be incorporated into the flap and taken with a short leash. We prefer to use the cutaneous vein for venous drainage because its size and caliber make microanastomosis straight forward.
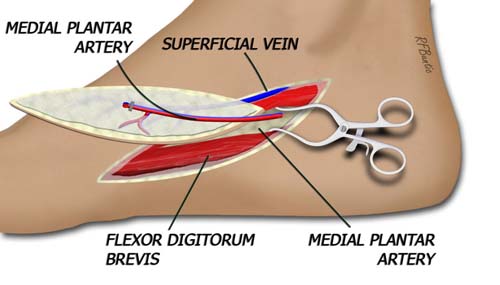
The flap is isolated on the deep artery and superficial vein.
Post Operative Care
The foot must be kept elevated to minimize edema. We allow ambulation with weight bearing when all eschar on the incision or skin graft has resolved.