Rectus Muscle Flap
Anatomic considerations
Anatomy
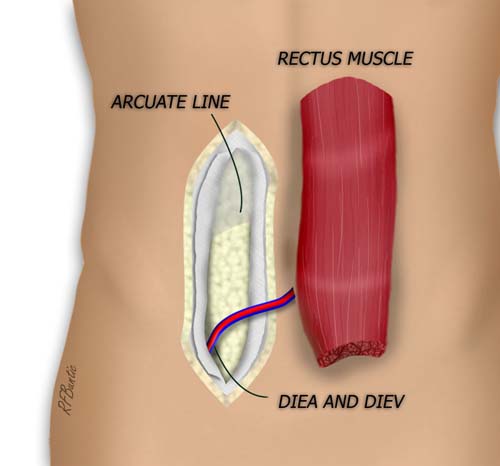
The paired rectus muscles provide abdominal flexion and support for the intra-abdominal contents. The origin of the muscles is the pubic symphysis and pubic crest, while the insertion is the fifth to seventh costal cartilages. The muscle is enclosed by the rectus sheath, but below the arcuate line, this sheath disappears posterior to the muscle. An important area of weakness that should be recognized when securing abdominal closure after flap harvest. The muscle can be up to 30 cm long and up to 10 centimeters wide.
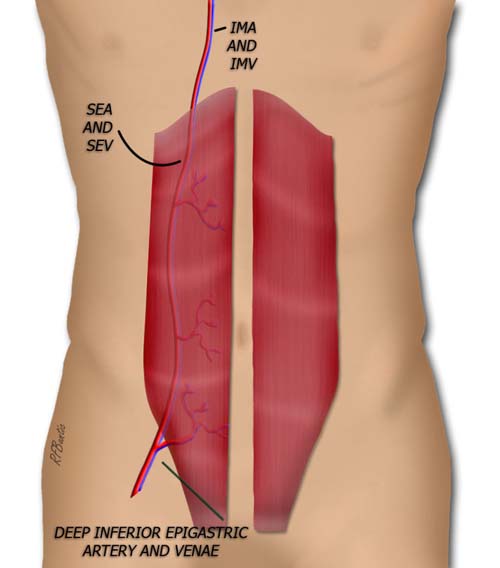
Each rectus is supplied by the deep inferior epigastric artery and drained by the deep inferior epigastric vein inferiorly. Superiorly, the inflow is via the deep superior epigastric artery and vein, and extension of the internal mammary artery inferior to the costal margin.
The Operative Procedure
The muscle can be exposed through a vertical or lower transverse incision. For ease of illustration and explanation the vertical incision is used here. It is placed off the midline, on the axis of the muscle. The total length of the incision depends on the amount of muscle to be harvested.

A vertical rectus harvest incision is pictured. As an alternative, the transverse incision may be used. See PMR flap.
The subcutaneous fat is divided down to the level of the rectus sheath. Perforators are ligated and divided. Cautery of the perforators may find the surgeon chasing them into the muscle and damaging the muscle.
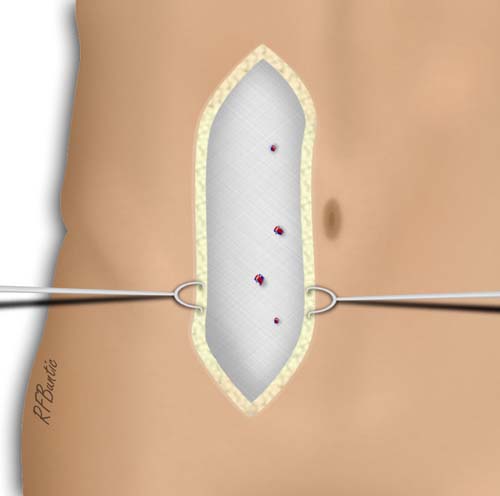
The rectus sheath is exposed. Small perforators to the skin are ligated.
The rectus sheath is divided longitudinally. Inscriptions make this division harder and care must be taken at the inscriptions. The fascia is elevated medially and laterally while gentle retraction is performed with Aliss clamps. Again the inscriptions are tightly adherent and must be teased off the muscle without damaging the muscle fibers.
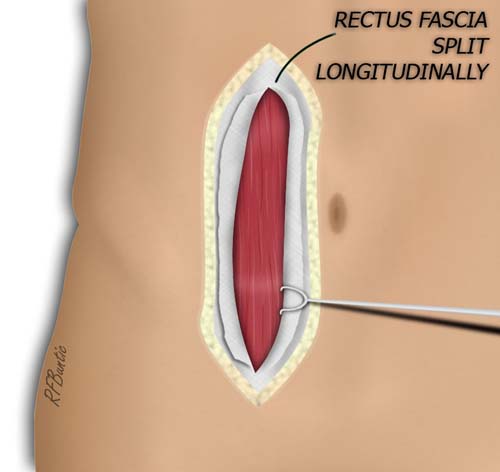
A longitudinal split is made in the rectus sheath. The sheath is elevated from the muscle. At the point of the rectus inscriptions, the sheath is adherent and required dissection with the electrocautery.
At the lateral inferior muscle, the thing fascial layer over the deep fat is divided and the muscle is gently retracted medially. The deep inferior epigastric artery and it's accompanying veins are identified. They can be traced down to their origin.
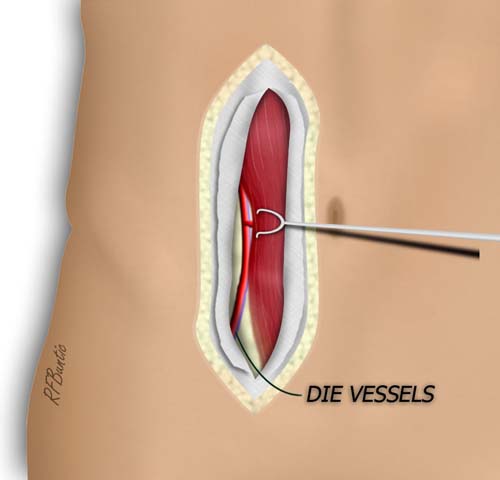
The pedicle to the rectus is identified by entering the areolar fat plane lateral to the muscle at it's inferior aspect.
The origin of the muscle near the pubis is isolated by encircling the muscle with the index finger. The muscle is then divided with cautery while protecting the pedicle. The superior muscle is likewise encircled and divided to isolate the rectus on the pedicle. The superior epigastric vessels must be securely ligated or cauterized to stop bleeding from the superior retracting muscle edge.
The muscle is isolated and the pedicle can be traced back to it's origin on the external iliac vessels.
The fascia is closed with running non-absorbable suture. If a large dead space is created above the fascia, as is the case in the transverse incision or often when skin paddles are harvested, then the wound should be drained.