Superior Gluteal Artery Perforator (SGAP) Flap
Anatomic considerations
The SGAP flap has been primarily used as an alternate for breast reconstruction, and requires significant microsurgical experience to harvest. The thickness of fat available provides volume for unilateral reconstruction, but positioning and the donor scar deformity have made this a less popular choice even among very experienced microsurgeons.
Vascular Anatomy
The superior gluteal artery and venae arise from the internal iliac system deep in the pelvis. They exit posteriorly through the greater sciatic foramen, superior to the piriformis muscle and inferior to the gluteus medius. The vessels perforate the gluteus maximus muscle on their way to the fat and skin that overlies them. The exit from the sandwich formed by the piriformis and the gluteus medius corresponds roughly anatomically to 6 centimeters below the posterior superior iliac spine and 4.5 centimeters lateral to the midline of the sacrum.
The exact position of the perforators is found by using the pencil Doppler to identify their course lateral to the exit of the artery from the pelvis.
The inferior gluteal artery and the sciatic nerve emerge inferior to the piriformis muscle, supplying the territory of the inferior gluteal flap.
The inferior gluteal artery and the sciatic nerve emerge inferior to the piriformis muscle, supplying the territory of the inferior gluteal flap.
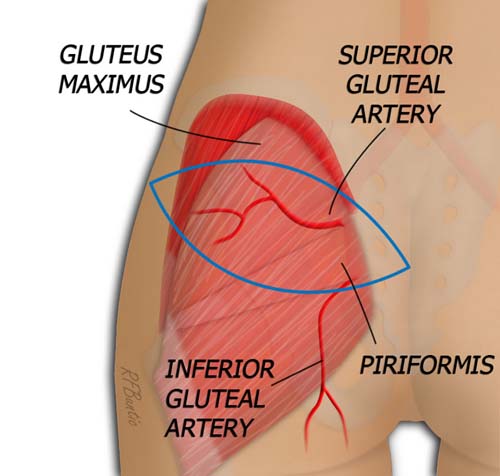
The superior gluteal artery exits between the gluteus medius and piriformis muscles.
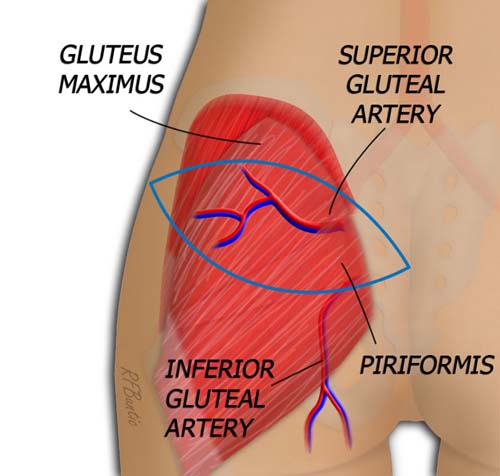
The superior gluteal artery and it's venae perforate the gluteus maximus to enter the subcutaneous fat of the flap.
Operative Procedure
The lateral decubitus position is used for a unilateral flap. The patient is placed prone for bilateral flap harvests.
The skin island of the flap is drawn overlying the superior gluteal artery perforators marked out by pencil Doppler exam. The flap is elliptical, an at roughly a 45 degree slant upwards from medial to lateral. The apex of the axis of the flap is marked beginning two to three finger breadths below the gluteal crease in the midline and extending laterally and superiorly to incorporate the perforator vessels. This allows for placement of the scar below many clothing variations. The flap can be designed from 6 to 13 centimeters wide and from 20 to 25 centimeters long. Surgical judgement must be used to ensure too much width is not taken a a defect is left behind that requires excessive tension for closure.
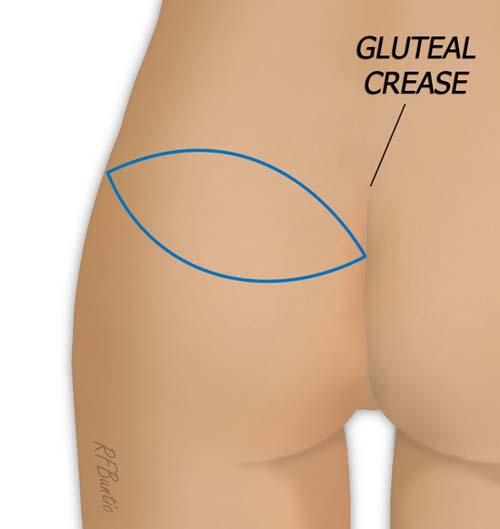
The orientation and position of the flap is marked. It begins medial two or three finger breadths below the upper aspect of the gluteal crease. It then angles superiorly and laterally as depicted.
The flap is elevated from lateral and superior toward the medial aspect, deep to the muscular fascia and above the gluteus maximus muscle. When the larger perforator(s) are identified as one proceeds medially, they are traced into the muscle with bipolar dissection and dissected to their exit from between the piriformis and gluteus medius muscles.
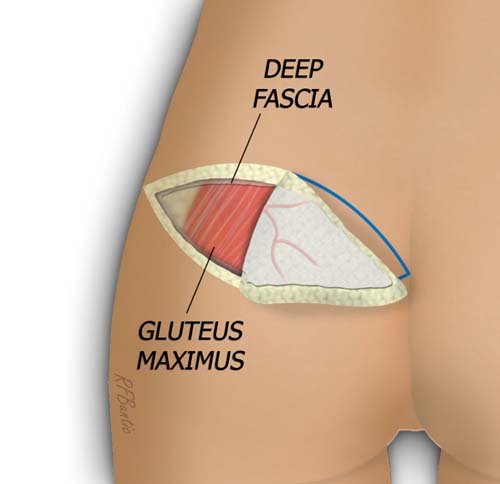
The flap is elevated from superior and lateral to medial, deep to the muscular fascia. The exit of the dominant perforator from the gluteus must be identified.
The medial and inferior incisions can be made and the pedicle traced more proximally by placing retraction between the exit of the artery and it's venae between the muscular space by separating the muscles from the vascular system. The artery and venae enlarge significantly in size at this point and there are multiple small branches emanating in all directions. They require careful ligation with bipolar electrocautery and/or hemoclips. Loss of proximal control of the vessels can be lead to significant bleeding and retraction of the vein into the pelvis.

When the dominant perforator(s) is found, it is traced through the muscle and between the piriformis and gluteus medius.
The donor area is closed in layers over a suction drain. The patient is placed post-operatively supine, and can have slight hip flexion. Ambulation is allowed in 3 to 4 days as the donor tension relaxes.