The Temporoparietal Fascia (TPF) flap
Anatomic considerations
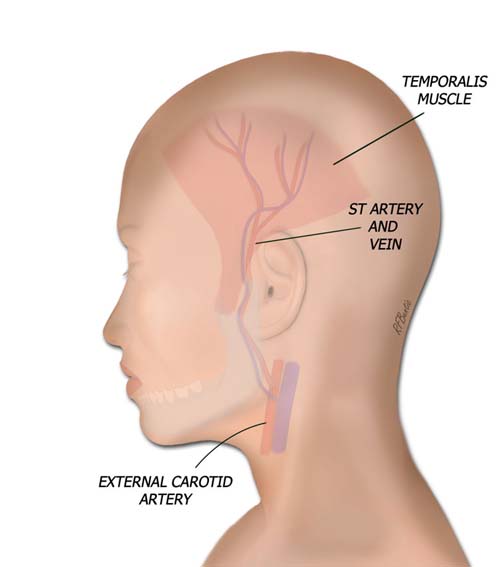
The temporoparietal fascia (TPF) is an extension of the subcutaneous musculoaponeurotic system (SMAS) inferiorly and the galea aponeurotica superiorly. It provides a thin sheet of vascularized fascia based on the superficial temporal artery and vein. The temporal muscle fascia lies deep to the TPF over the temporalis muscle. Above the temporalis muscle, the pericranium and skull lie deep to the TPF.
Vascular Anatomy
The blood supply of the TPF flap is from the superficial temporal artery and vein. The artery is a branch of the external carotid system. It travels with the vein anterior to the ear where a pulse can be easily palpated. The artery gives off numerous branches as it ascends, including branches to the ascending helix of the ear, the temporalis muscle, and the anterior, middle and posterior TPF and scalp.
The frontal branch of the facial nerve runs on a line from a point just inferior to the tragus to the lateral brow and will come into play if the dissection is carried too deep. The auriculotemporal branch of the maxillary nerve lies posterior to the artery and provides sensation to the scalp. It is usually divided during elevation of the flap, forming and insensate are on the lateral scalp.
The temporoparietal fascia flaps is supplied by the superficial temporal artery and vein. The fascia is superficial to the deep temporal fascia, and just below the hair follicles of the scalp.
Operative Procedure
The skin incision is placed anterior to the ear, in the preauricular crease if desired. It divides into a "Y" shape superiorly, allowing for wide exposure of the flap. If a narrower flap is desired, a simple linear incision can be made superiorly.
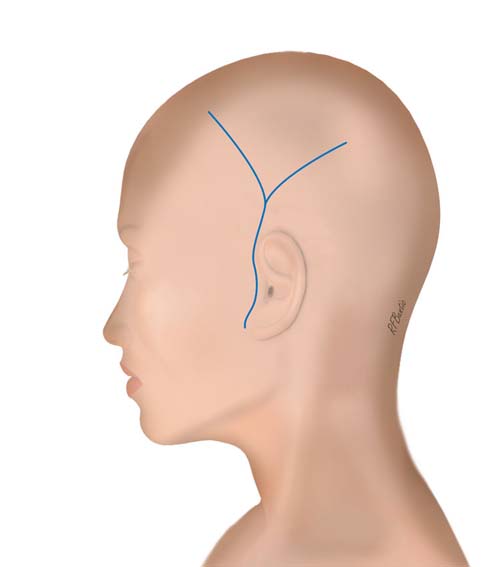
The incision is in the preauricular area and is fashioned in a "Y" shape in the scalp, to allow for exposure of the fascia.
The skin is elevated just deep to the dermis, taking care to avoid injury to the vein, which runs superficial to the artery. In the scalp, the skin is elevated just at the level of the junction of the hair follicles and the STF. The connection between the scalp and the TPF is firm, and requires sharp dissection with a knife and an assistant that follows along with the bipolar cautery to coagulate small blood vessels.
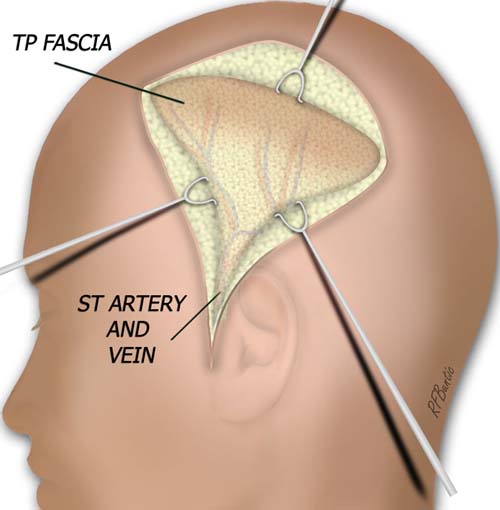
The skin flaps are elevated just deep to the hair follicles, with care being taken not to amputate the follicles. The dissection is usually done sharply with a knife, while the assistant follows with bipolar electrocautery.
After the anterior and posterior flaps are developed in the scalp, and the pedicle is identified anterior to the ear, the flap is incised along its superior periphery.
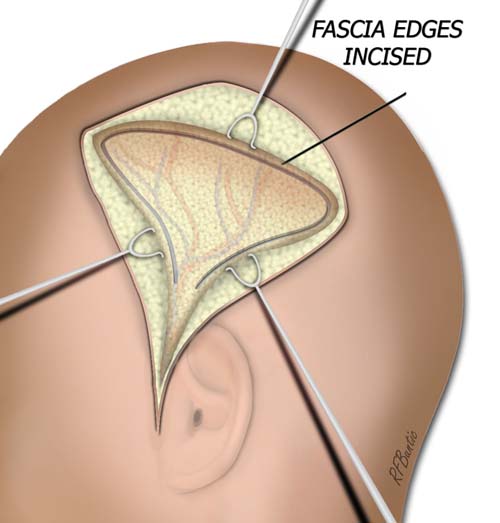
When the skin flaps are elevated, the superior aspect of the STF flap is incised down to the deep temporal fascia.
There is a loose, areolar plane over the skull and temporalis muscle fascia that allows the flap to be raised from the deep fascia quite easily. The flap should be narrowed as one proceeds near the frontal branch of the facial nerve, so as not to transect the innervation to the muscles of the forehead.
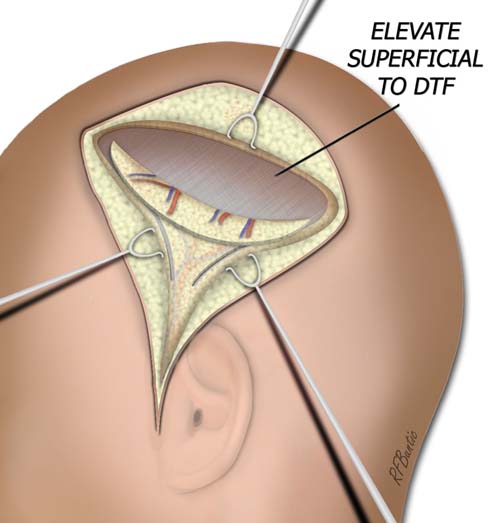
Elevation at this level is quite quick, where an areolar plane separates the deep temporal fascia from the superficial temporal fascia.
The flap is elevated to the pedicle anterior to the tragus and isolated on the artery and vein.
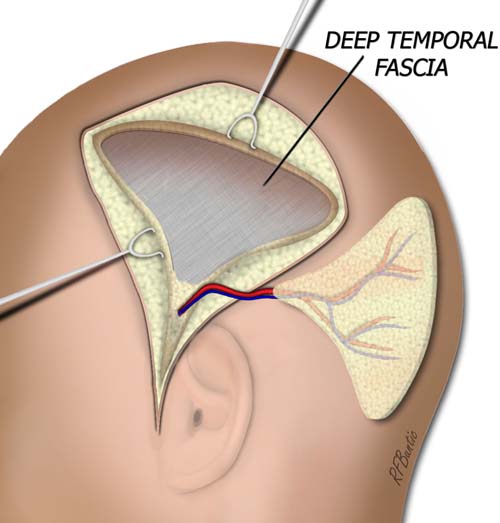
The flap is isolated on the vascular pedicle.
Post-Operative Care
The scalp incisions are closed over suction drains and the preauricular incision is closed with fine suture in a face lift fashion. The head is then dressed with gentle pressure using kerlix rolls over cotton.