The Transverse Upper Gracilis (TUG) Flap
Anatomic considerations

Anatomy
The cutaneous perforators of the gracilis muscle supply both the anterior and posterior inner thigh skin reliably. The transverse orientation of the flap allows for a large skin paddle, with some independence from the muscle below.
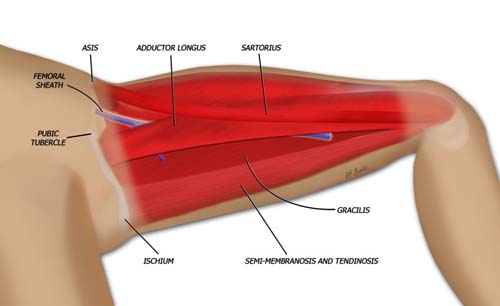
The perforator for the transverse upper gracilis flap travels through the gracilis muscle. The muscle is small and expendable, with no resultant hernia formation or bulging after removal.