The Partial Superior Latissimus(PSL) Flap
Anatomic considerations
The partial superior latissimus muscle provides a long pedicle and large, thin muscle that can be innervated. The lateral aspect and innervation of the latissimus muscle are spared, preserving lateral muscle function and the dorsal thoracic silhouette. The flap can cover both large and small defects and provides a very long vascular leash, allowing reconstruction of complex deformities
Anatomy
The partial superior latissimus muscle relies on inflow from the transverse branch of the thoracodorsal artery. The branch arises intramuscularly, after the thoracodorsal vessels and nerve enter the muscle on it's deep surface in the posterior axilla.
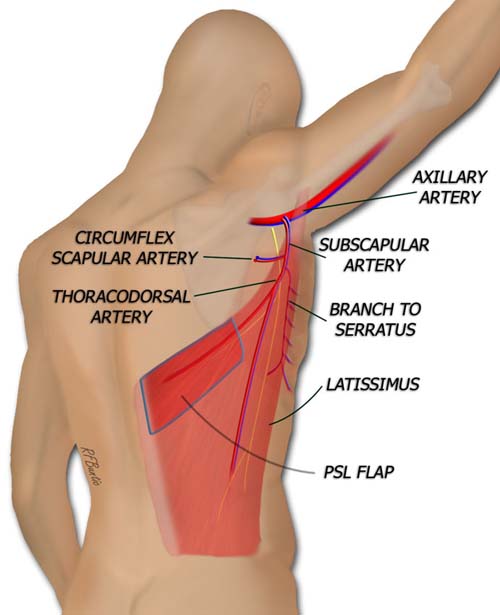
The partial superior latissimus muscle flap is supplied by the transverse branch of the thoracodorsal artery. A nerve accompanies this branch. The descending branch of the nerve is spared in the flap harvest, leaving the lateral muscle innervated.
Flap Dissection
The patient is positioned and prepped similar to a latissimus muscle harvest. The inferior angle of the scapula is palpated and guides the surgeon to the superior extent of the latissimus muscle. The incision is drawn a finger breadth or two inferior to this, along the axis of the fibers of the upper latissimus. A skin paddle can be designed over this muscle.
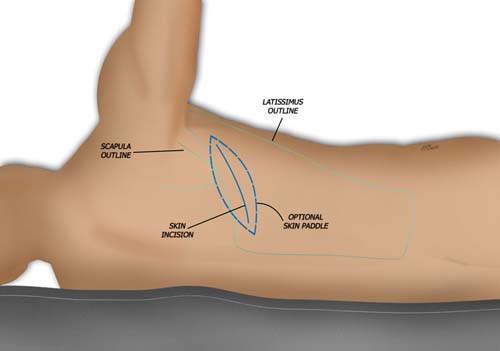
The flap marking are identified by outlining the latissimus muscle and scapula. The incision is made near the upper border of the latissimus. A skin paddle is optional, and best designed by locating a dominant perforator with a pencil Doppler.
An inferior skin flap is created superficial to the muscle. The upper border of the latissimus is identified and the muscle is then retracted away from the chest wall, to expose the undersurface. The dissection proceeds toward the axilla, and the thoracodorsal artery and accompanying vein are identified as they enter the muscle. The pedicle is freed proximal to entry point, and the transverse and descending branches of the artery are identified. The descending branch of the nerve must be spared to preserve innervation to the lateral muscle.
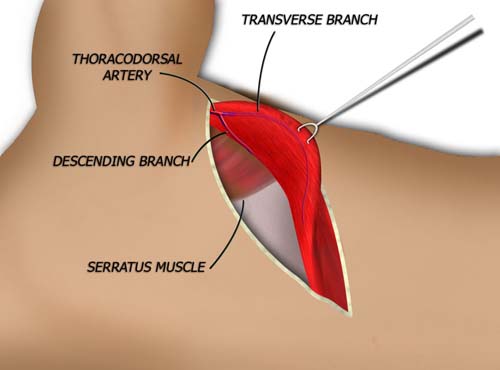
The muscle is elevated from the chest wall and retracted away from the chest and inferiorly to identify the transverse artery branch. This branch is best seen entering the muscle laterally, toward the axilla.
A marking pen is used to outline the extent of the PSL flap and the muscle dissection is performed with scissors and the bipolar electrocautery. If a long pedicle is desired, the artery is traced to the subscapular origin on the axillary vessels.
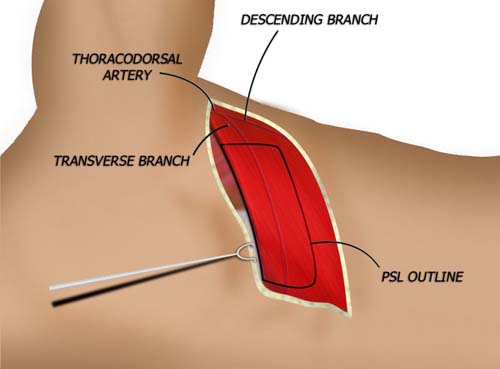
The extent of flap harvest can be outlined with a marking pen. The medial and inferior incisions are made first. The pedicle to the flap is identified laterally and the muscle of the lateral flap is divided, sparing the pedicle.
The skin defect is closed in layers over a suction drain.

The harvested partial superior latissimus. The pedicle can be traced to the subscapular artery to gain tremendous length.
Postoperative Care
We allow the patient to use the ipsilateral arm postoperatively and no special dressings are required. The donor area should be inspected daily for hematoma formation. This donor area can form a seroma, necessitating drains.