The deep inferior epigastric artery perforator (DIEP) flap
Anatomic considerations
The DIEP flap can be used for a variety of reconstructive procedures when a large segment of soft tissue, including fat and skin is necessary. It has become more popular for breast reconstruction, but requires significant microsurgical experience to harvest.
Anatomy
The deep inferior epigastric artery arises from the external iliac artery and runs from lateral to medial under the rectus muscle. It can enter the substance of the muscle or run deep to it, while sending branches into the muscle and through the muscle. Perforators often travel through the tendinous inscriptions of the rectus muscle, making their dissection somewhat more difficult. In most patients the DIEP and its venae can supply adequate circulation for zones 1-3, making the territory of perfusion larger than that of the SIEA flap.
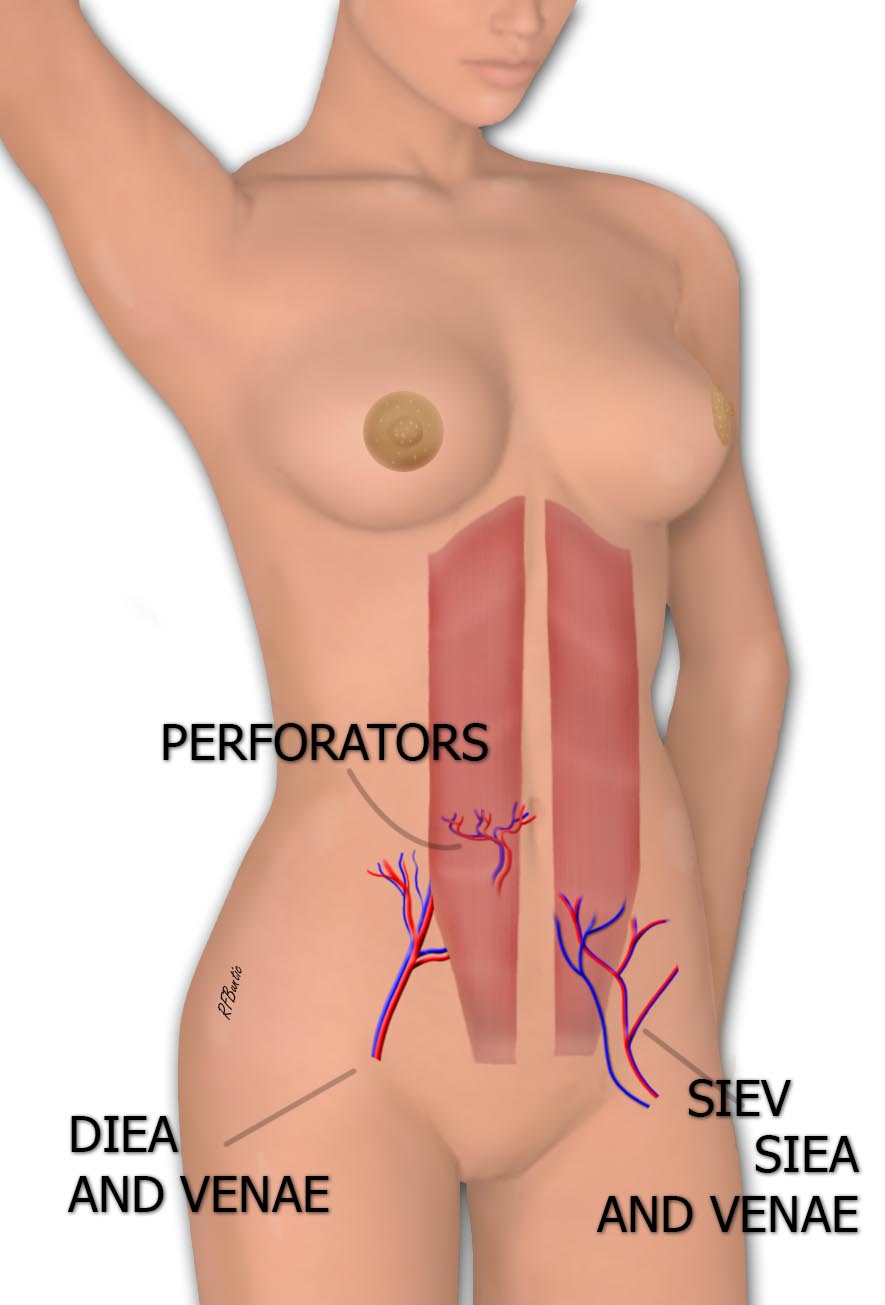
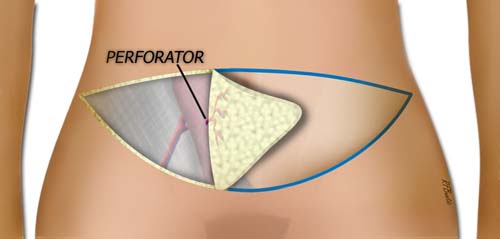
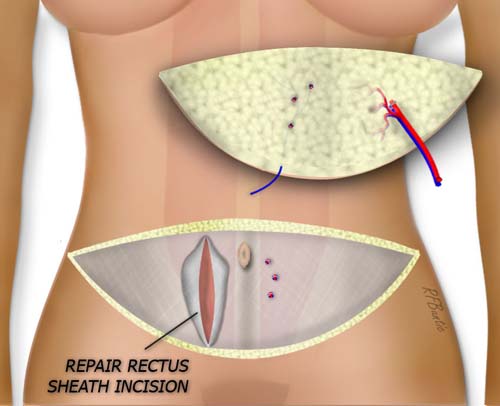
Anatomy of the abdominal skin harvested with the DIEP flap. On the right side of the abdomen, a large DIEP perforator through the rectus muscle is illustrated. On the contralateral side, the superficial inferior epigastric artery (SIEA) and the superficial inferior epigastric vein (SIEV) are demonstrated. Both the DIEP and SIEA system provide circulation to the lower abdominal skin. However, the SIEA is usually small and has a shorter vascular leash. Most surgeons prefer the DIEP flap is available.
The perforating branches pierce the rectus fascia to supply the abdominal fat and skin. The DIEA and the accompanying veins are pictured in the illustration entering the muscle below the junction of the middle and lower third of the muscle. The DIEA can run laterally, medially or centrally under the muscle, as it ascends superiorly. There often is symmetry with the contralateral vessels, however this is not consistent.
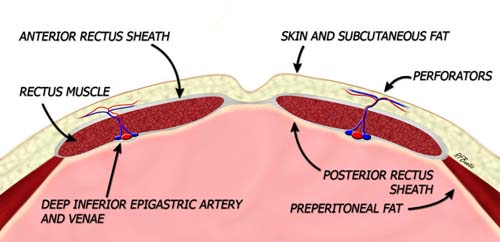
Cross Section of the abdominal wall demonstrating DIEA perforators. In this case a central DIEA system is shown with a perforating system piercing the rectus muscles and supplying the overlying skin and fat.
Flap Design
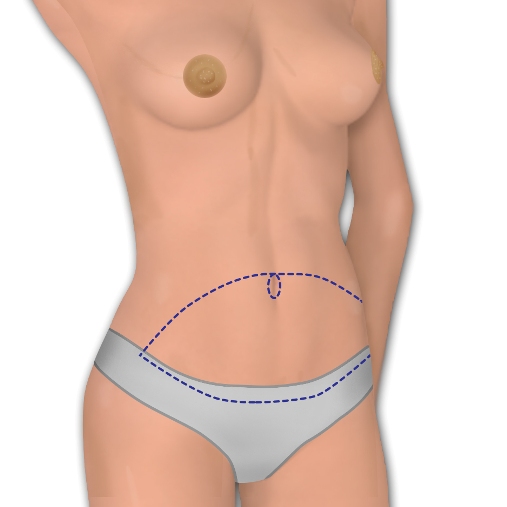
The abdominal skin island is designed with the lower aspect of the incision transversely placed above the pubic bone, in line with the typical transverse Cesarean section incision. It extends laterally with a gentle curve superior to the inguinal ligament finishing adjacent to the anterior superior iliac spines. The upper incision is placed above the umbilicus and gently curves laterally to meet the lower transverse incision marking. With the patient in the supine position and the knees slightly flexed.
After flap harvesting, the abdominal skin and fat above the flap is elevated to the costal margin (green arrows). The tissue plane is just superior to the rectus sheath, centrally it is firmly attached to the rectus sheath while laterally this plane is quite mobile. By beginning the elevation laterally and then focusing medially, the elevation is simpler.
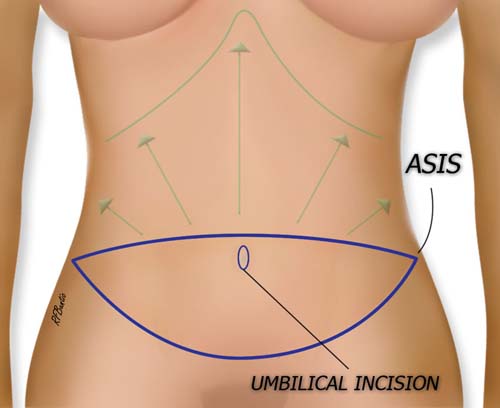
The green arrows show the extent of undermining after flap harvest to close the abdomen. A preoperative pinch test with the knees flexed can help assess the extent of the flap markings so closure is not too tight.
Operative Procedure
The patient is prepped and draped supine with the arms stretched out on an arm board. The abdominal tissue can be pinched to determine the tightness of postoperative closure and markings can be adjusted accordingly. This is best done with the knees and hips slightly flexed. Perforators can optionally be assessed with the pencil Doppler. If bilateral flaps are to be harvested, the Doppler signals can be marked on the contralateral side as well. This is a good practice even in unilateral flaps to find the largest and loudest perforators.
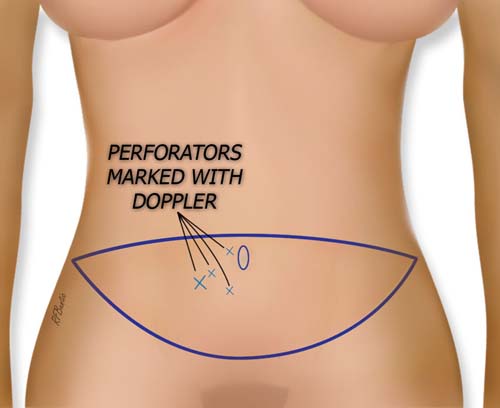
The flap is marked and the loudest Doppler signals are marked with an "x". The loudest perforator is marked with largest size "x". This is the perforator that is dissected free in the illustrations below.
The flap is usually elevated from lateral to medial and the search for perforators is begun when the territory of the rectus sheath over the lateral rectus muscle is reached. This dissection can be performed with the electrocautery on a low setting, or with bipolar forceps and scissors. If bilateral flaps are being prepared, the midline incision can be made and the flap traced from medial to lateral as well, in order to help surround the perforators. Note that the attachment of the flap to the rectus fascia in the midline is much more adherent and the plane is more difficult to dissect at this level.
The major perforator to the skin is identified. In this case there is one major perforator and it is used for the flap harvest.
As larger perforators are identified, smaller ones may be ligated. Usually the single flap can be supported on one major perforator. Occasionally, if the perforators are small, a second perforator may be used as well, as long is it is in a similar longitudinal plane with its counterpart. Two different longitudinal planes would result in excess muscle transection. The whole point of the DIEP flap is to preserve abdominal muscles.
The umbilicus is separated from the flap with a periumbilical incision (marked in blue above), leaving the stalk attached to the abdominal wall. When the abdomen is re draped, the umbilicus is brought through an new incision.
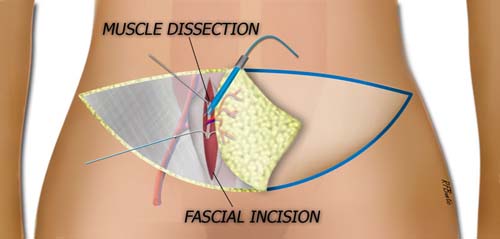
The facia is incised longitudinally and the perforator is traced through the rectus muscle. Very small branches to the muscle are ligated or coagulated with the bipolar electrocautery.
When a large dominant perforator is isolated, the rectus fascia is incised longitudinally, around the perforator. Great care is required so as to not injure the vessels, especially the vein, which can be quite delicate. The fascia is opened for 10 to 12 centimeters and the perforator is traced through the muscle, using gentle retraction of the muscle and the bipolar electrocautery. Small branches of the perforator are coagulated or clipped as they sprout into the muscle and the perforator is traced to the DIEA and the venae commitans.
The perforator is approached from medial and lateral and isolated to the DIEA and veins. It is "surrounded".
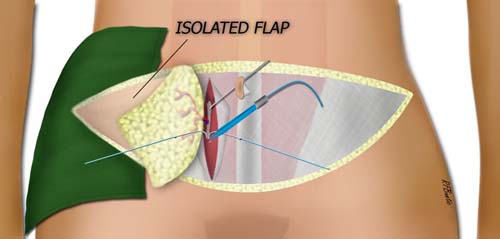
The DIEA vessels are then traced back to near their origin while retracting the muscle away from the deep abdominal contents. When the entire flap is isolated on the perforator and DIEA/DIEV, and the recipient area is ready, the DIEA and the venae can be ligated and divided. The rectus sheath is closed with a running large caliber non-braided suture.
The flap is isolated on the DIEP vessels. In this case the contralateral superficial vein was also harvested.
The abdominal wall is undermined to the costal margin and the abdominal incision is closed in layers over suction drains with the hips flexed and knees bent in a semi-Fowler position. The umbilicus is brought through the abdominal wall and sutured into position. The patient is allowed to mobilize when clinically indicated for the recipient area. The patient ambulates with the hips flexed until the tension of the closure slowly resolves.