Partial Medial Rectus (PMR) Flap
Anatomic considerations
Anatomy
The partial medial rectus flap provides a small- or medium-sized muscle with blood supply provided by branches of the deep inferior epigastric artery and it's venae. For a long pedicle, the deep inferior epigastric artery can be dissected to the origin on the external iliac artery. Although flap design is straightforward, intramuscular dissection is necessary, similar to the technique required when tracing perforator vessels through a muscle, such as in the DIEP or intramuscular ALT flap. Only a portion of the rectus is taken, and the lateral muscle is left in continuity, leaving functional muscle behind to aid in abdominal wall strength.
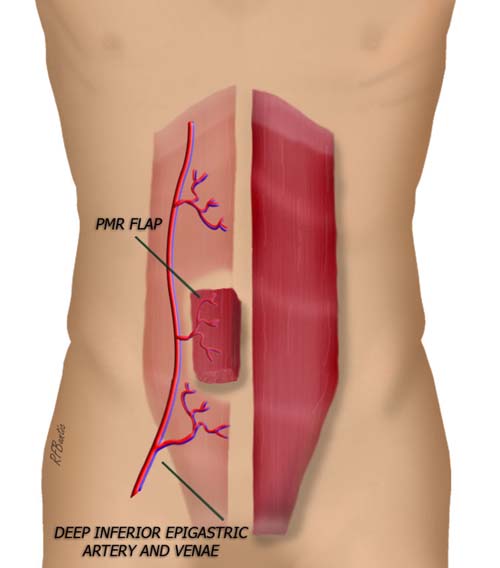
The flap is fabricated using a portion of the medial rectus muscle. The blood supply to the medial rectus is variable, but the flap can be elevated regardless of the vascular inflow pattern.
The Operative Procedure
A transverse lower abdominal incision is used, keeping the scar in the suprapubic crease. This provides for a more aesthetic donor site outcome and avoids the vertical highly visible scar.
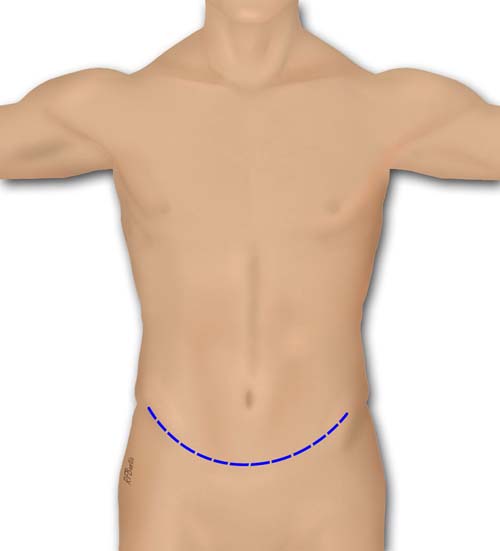
A transverse lower abdominal incision is used. This helps to conceal the scar and is more aesthetic than a vertical incision.
The abdominal wall is elevated superficial to the rectus fascia, like an abdominoplasty. Perforators are ligated or coagulated and the rectus fascia is exposed where the muscle harvest is to be performed. If a longer pedicle is desired, the muscle can be harvested higher up, in which case the stalk of the umbilicus can be transected and then re-attached at time of closure.
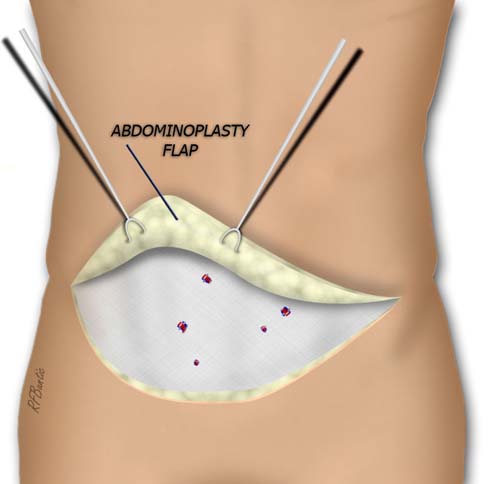
The lower abdominal wall is elevated superficial to the rectus fascia
A vertical incision is made in the rectus fascia over the central or medial muscle. The deep inferior epigastric vessels can be visualized if desired, but we do not usually dissect laterally superficial to muscle.
The medial rectus muscle is exposed. Looks for the deep inferior epigastric vessels laterally is optional.
An area is outlined with a marking pen, depending on the size of muscle necessary in the recipient area. Remember that the muscle will contract when transected and get wider.
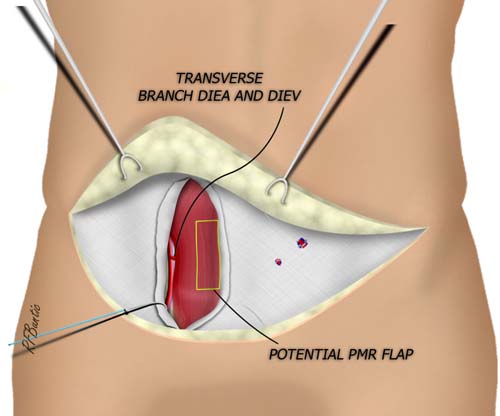
The flap area is outlined in yellow. The longitudinal line is split to identify transverse branches to the medial muscle.
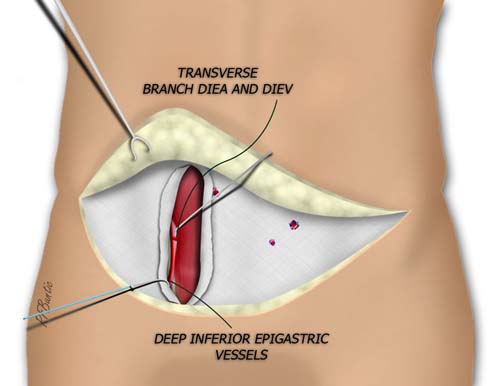
A split is made in the rectus muscle longitudinally, sparing transverse vascular branches. A large transverse vessel is found, or the deep inferior epigastric artery may be right below or medial. The flap may be redesigned superiorly or inferiorly if the nourishing branch is high or low.
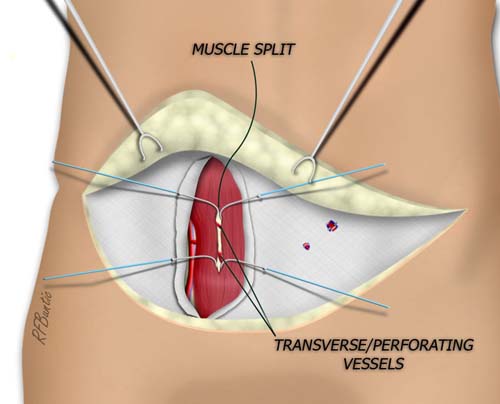
The transverse branches to the medial muscle are found. The largest branch is used to peruse the flap. This branch is then traced to its origin on the deep inferior epigastric vessels.
After the vascular branches are found, the superior and inferior part of the flap are transected. We usually perform this with the bipolar electrocautery.
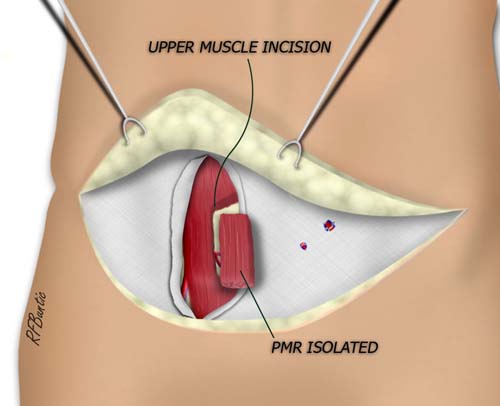
The superior and inferior flap are transected and the flap is isolated on the deep inferior epigastric vessels.
The pedicle of the flap is then traced as long as needed. We picture it here below passed laterally under the muscle. It does not need to be passed laterally.
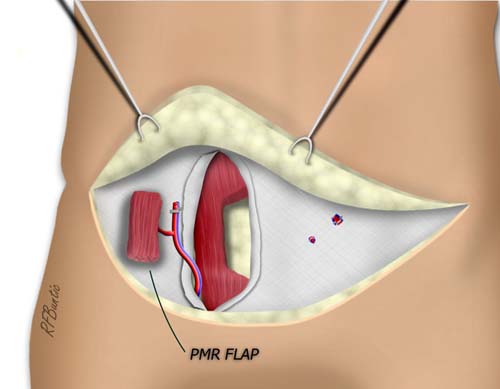
The flap can be passed underneath the lateral rectus to gain pedicle length to the origin of the deep inferior epigastric vessels on the external iliac system.
Suction drains are placed and the wound is closed in layers. If desired, a mini-abdominoplasty can be performed and the resected skin can be used for the skin graft.