The transverse upper gracilis (TUG) flap
Not all patients are who researching breast reconstruction are candidates for using abdominal tissue, and some who are may not want to have scars on their abdomen. Fashionable jeans and workout sweats can reveal lower tummy skin an even the belly button, and some women may prefer this style and worry about the abdominal scarring with a DIEP flap. In addition, very thin or athletic patients may not have enough abdominal subcutaneous fat present to be a candidate for SIEA or DIEP breast reconstruction. Some women may have had a previous tummy tuck or abdominal surgery that precludes breast reconstruction with abdominal fat. There are other options for autolgous reconstruction.
The gracilis muscle and the overlying skin have been used for many years in reconstructive microsurgery. These flaps have been used reliably to reconstruct cancer or traumatic defects in numerous different circumstances. Our appreciation of the TUG flap began with a report on the technique by Dr. Thomas Schoeller, who reported his findings using the TUG flap in patients that did not have an appropriate abdominal donor sites. The Austrian surgeon made a a great impression on us, because we were very impressed by his aesthetic results. We begun applying this procedure in the United States. Like all microsurgeons, we constantly strive to improve our results and we have added many modifications to this flap and believe it to be an excellent choice for breast reconstruction, often better than even SIEA or DIEP reconstruction. Many patients that lack the abdominal bulk to reconstruct a breast have enough inner thigh skin for a reconstruction.
The ideal donor area should have enough fat to reconstruct a breast, while having a consistent blood supply. Ideally it should not result in side effects like functional loss or hernia formation. In many patients, tissue from the inner thigh can be used to reconstruct a breast. This area of the body has a consistent blood supply, is well known to most microsurgeons, and does not lead to hernia formation or significant functional loss. The flap is sometimes known as the transverse upper gracilis (TUG), although this can be misleading since the flap as originally described for other forms of reconstruction has been modified to reconstruct breasts. We prefer the term Inner Thigh Flap.
Tissue from the inner thigh has a significant amount fat of that can be sculpted to form a breast. In some respects, this tissue is ideal for sculpting and can mimic the contour of a breast more closely than the abdominal tissue. The TUG results in removal of tissue that is discarded in the cosmetic medial thigh lift operation (removal of inner thigh fullness or sagging). Along with this tissue, part of the gracilis muscle is removed. The much larger thigh adductor muscles are stronger than the gracilis and removal of this portion of gracilis muscle results in no measurable functional loss. Unlike loss of muscle in the TRAM flap, loss of the gracilis muscle does not result in hernia formation or bulging afterward. The muscle is small in comparison to the rectus and supplies only an accessory role in forcefully bringing the thighs together. This is in contrast to the rectus muscle of the TRAM flap, where abdominal wall weakness and hernia can result.
We have removed hundreds of gracilis muscles from patients with no functional loss or hernia formation. In many ways, use of the inner thigh flap results in the aesthetic perk of a thigh lift. If followed several months later by lateral thigh and hip liposuction, women with relatively large thighs can have their thighs slimmed down significantly. The gracilis muscle and the overlying skin have been used for many years in reconstructive microsurgery. These flaps have been used reliably to reconstruct cancer or traumatic defects in numerous different circumstances. Our interest in TUG reconstruction developed after seeing the results Dr. Thomas Schoeeler presented at an American Society for Reconstructive Microsurgery (ASRM) meeting. Dr. Schoeeler, an Austrian, presented his findings using the TUG flap in patients that did not have an appropriate abdominal donor sites. Because we were very impressed by their report we have begun applying this procedure in the United States as it applies to breast reconstruction.
Although the TUG flap is not performed widely in the United States, we believe this reconstruction is an excellent choice for many patients and provides some of the best aesthetic results we have seen. The unique shape of the tissue removed from the inner thigh allows shaping of a breast with an almost ideal contour and projection. And, this flap uniquely provides the potential for immediate nipple areola reconstruction without tattooing.
We have been proponents of the TUG flap because of the many advantages it has. These advantages include:
- Superior breast shaping
- Immediate nipple areolar reconstruction in some patients
- Consistent and excellent blood supply
- Inner thigh lift
- A high success rate with skilled microsurgeon
- Can be used in immediate or delayed reconstruction
The tissue from the inner thigh is removed with some underlying skin, fat and expendable gracilis muscle. The flap is then sculpted to a circular shape with some conical projection. This is outlined in figures A, B and C below. The flap as it is shaped in C can be placed in the breast pocket of the mastectomy, and circulation is reestablished microsurgically to the internal mammary blood vessels. Just like in the DIEP and SIEA procedures further shaping is done to match the opposite breast as closely as possible. Superior results can be obtained with immediate reconstruction and skin sparing mastectomy
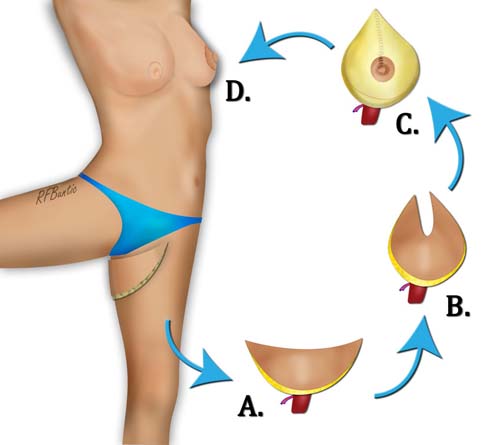
The TUG flap breast reconstruction uses inner thigh tissue that is shaped into a breast mound.
Sculpting of the TUG Flap
The crescent shape of the TUG flap allows it to be shaped by coning, giving it projection, and a rounder appearance. The projection is superior to that created by DIEP and SIEA flaps, and gives a more natural contour to the new breast. By using the crescent shape and folding to full advantage, the nipple areola structure can be created. The natural darker color of the inner thigh compared to the relatively pale breast color, give the areola superior shading of skin than can be obtained with tattooing.
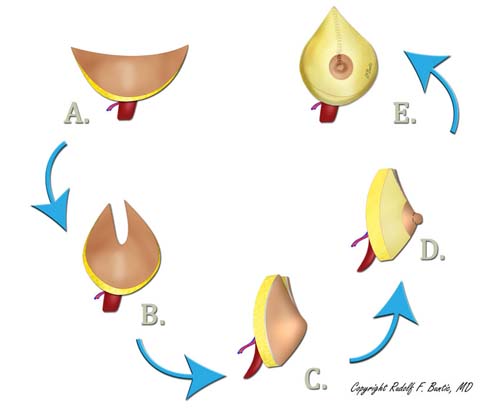
The flap is sculpted into the shape of a breast, with the crescentic shape resulting in a form that mimics the breast better than the flatter tissue of the abdomen.

The TUG flap donor area leaves a scar on the inner, upper thigh.
The inner thigh lift is performed during the reconstruction, with the thigh wound closed under some tension. The patient is asked not to abduct (spread apart) their legs for several days. Over the course of the in hospital stay, the tension on the incision site begins to soften and the patient resumes a recovery similar to the DIEP or SIEA flap patient.