DIEP Flap Microsurgical Breast Reconstruction
The DIEP (deep inferior epigastric perforator) flap was first described in 1991 by a Japanese microsurgeon. But, it wasn't until 1994 when Robert Allen reported that he had applied this flap to breast reconstruction that it was demonstrated what a big advantage the DIEP was over the TRAM flap. Dr. Allen was the first to recognize the benefits of this kind of reconstruction, and along with the Belgian surgeon Philipe Blondeel, he convinced a number of microsurgeons that the extra time, care and skill needed for this surgery was well worth the effort.
The DIEP flap provides the necessary tissue for a breast reconstruction while sparing the loss of the rectus muscles and fascia. This provides the DIEP flap with significant benefits over the TRAM reconstruction. Yet the TRAM is still the much more common abdominal tissue breast reconstruction technique.
According to American Society of Plastic Surgeon statistics, implant and expander reconstructions were more than 20 times more common that DIEP flap reconstructions in 2006. TRAM flaps were twice as common as DIEP flaps. No data was available on SIEA and TUG reconstructions, which are much less common.
With the DIEP, patients have less post-operative pain, less post-surgical abdominal wall weakness and a decreased chance of abdominal wall hernia formation. By preserving the abdominal muscles, potential complications and loss of strength can be reduced. Since this type of reconstruction is not offered by all plastic surgeons, many patients are under the impression that this is a very new procedure. However, DIEP flaps have been done for many years now and have been confirmed to be an excellent option for breast reconstruction.
Many women are frustrated by the lack of availability of these flaps. Unfortunately, the technical skill and training demands for this procedure are steep, and for this reason it is unlikely that it will ever be widely available. Most plastic surgeons find it much easier to perform the TRAM, latissimus flap or implant reconstructions.
Detailed Information
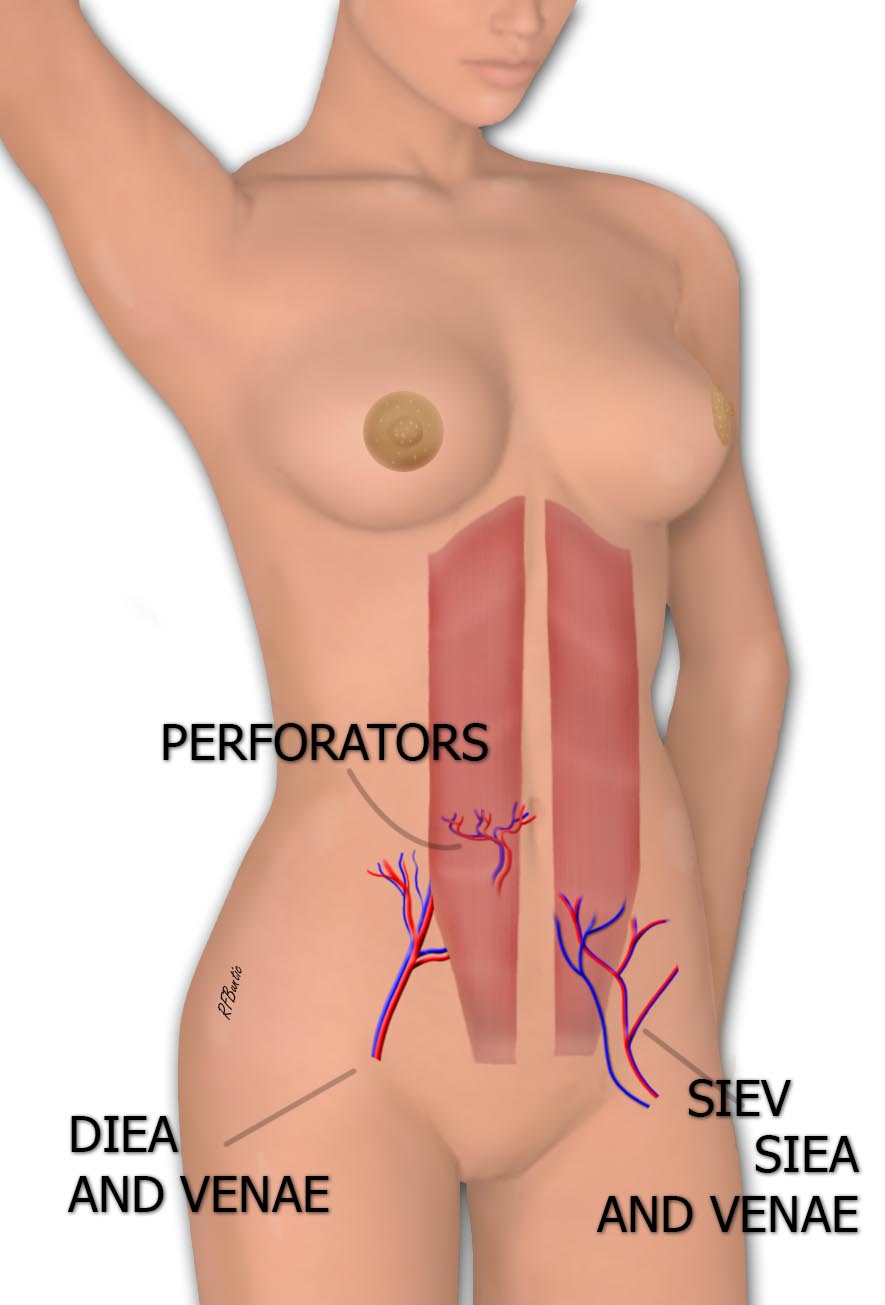
The DIEP flap relies on blood vessels that travel through (perforate) the rectus abdominus muscle to supply the overlying abdominal skin. The vessels that supply the perforator circulation to the flap are the deep inferior epigastric artery and the deep inferior epigastric vein. Hence, DIEP is an acronym for 'deep inferior epigastric artery and vein perforator'.
The DIEP flap can be used for immediate or delayed reconstruction.
For those who like to know almost every detail and are interested in the more technical aspects of the surgery (usually engineers or physicians), we outline them here. The flap is elevated from the abdomen while circulation to both halves is preserved. We inspect for the presence of SIEA vessels (next chapter) and if present and adequeate, we proceed with SIEA flap harvest. If the SIEA vessels are not present or if they are too small to use, we dissect the DIEP vessels. For a single breast reconstruction we use approximately one-half of the lower abdominal skin and discard the side we find less favorable in terms of vessel size and vessel orientation. If two breasts require reconstruction, both lower halves are used, one for each reconstruction.
The DIEP flap exploits the abdominal skin and subcutaneous fat without sacrificing the rectus abdominus muscles or rectus sheath fascia. In contrast, fascia and muscle removal are performed in the TRAM flap. The so called muscle sparing TRAM (ms-TRAM) has proponents, but this procedure still involves muscle and fascia excision, and in our experience, is not necessary. In addition, the extent of muscle excision in the ms-TRAM is certainly variable from surgeon to surgeon and by procedure, and in our opinion, it is a surgery that lacks quantifiable standards of muscle and fascia excision. Surgeon to surgeon extent of muscle and fascia excision is currently not measurable. On the other hand, a DIEP is a DIEP and an SIEA is an SIEA. No interpretation is necessary.
Advantages of the DIEP flap include:
- Preservation of the rectus muscle
- Preservation of the rectus sheath
- Less post-operative pain compared to the TRAM
Because they are technically more complex than implant and TRAM flap surgery, DIEP/SIEA/TUG microsurgical reconstruction should only be performed in medical centers that routinely perform microsurgery.

The abdominal tissue used in the DIEP flap is outlined in blue.
Tissue from the abdomen, outlined in blue in the illustration above, is used to reconstruct the breast. After this tissue is transplanted to reconstruct the breast, a tummy tuck is performed.
DIEP Reconstruction in Greater Depth
The tissue used for DIEP breast reconstruction contains skin, fat and blood vessels. It is the same tissue area that is discarded in the classical cosmetic surgical abdominoplasty - also known as the tummy tuck.
The DIEP blood vessels run under the rectus muscle and through it.
The area outlined in blue on the abdomen represents the amount of abdominal skin that typically is used in DIEP flap breast reconstruction. The paired rectus abdominus muscles are illustrated in dark red. They are the muscles that give the abdomen strength and are the major generators of force in the sit-up. Their outlines are seen in physically fit individuals as a "six pack". The blood vessels are pictured that supply ciruculation to the abdominal tissue. These vessels pierce throught the muscle. In a TRAM flap, the muscle is taken to avoid dissection of the vessels. In the DIEP flap the muscle is operated on but not removed. A major advantage of the DIEP flap is that it does not result in the loss of the rectus abdominus muscles. The tissue that is removed is then sculpted to make a breast with new circulation. The area of the abdomen from which the tissue is removed is tightened as a result of the loss of excess skin. This is the component that is known as a tummy tuck.

The flap is removed from the abdomen and transferred to the chest
Microsurgery restores circulation to the tissue

Microsurgery is used to re-establish the circulation to the tissue
In the figure above, the flap has been moved into the mastectomy field and the vessels are microsurgically repaired to branches from the internal mammary artery and vein. To access the internal mammary artery and vein a portion of rib cartilage is removed from the chest wall. The microsurgery is done through the mastectomy scar, but the picture here shows the details directly over the ribs to explain the procedure visually.
Flap Sculpture
Shaping of the breast is done before and after the microsurgery is performed. There are many issues that contribute to the ultimate contour, and they include:
- The shape and possible need for further surgery on the other breast
- Skin sparing incisions
- Immediate reconstruction
- Delayed reconstruction
- Old scars
- Radiation
The most significant factor is the technical skill and artistic sense of the surgeon. Without excellent technical skill and the eye of an artist, results can range from failure to an aesthetically displeasing outcome.


Above, illustrations of the results with skin sparing mastectomy (left) and a delayed reconstruction (right). The abdominal skin island present on the breast is smaller for the immediate than the delayed reconstruction. The nipple areola reconstruction is usually scheduled for a later date, when all tissue has healed. Secondary revision surgery may be required on the breast to improve appearance or symmetry and depends on patient body type and desires. Later revisions are sometimes done in conjunction with abdominal scar revision.