Greater Omentum Flap
Anatomic considerations
In 1972 Harry Buncke and Donald McLean published results of the first successful clinical microsurgical transplant. They used the greater omentum to cover a large scalp defect with exposed cranial bone resulting from a post-traumatic defect. This achievement was built upon laboratory research in microsurgery, using one of the first operating diploscopes in the United States, and microsurgical suture that was created by directly bonding nylon on a handmade needle.
The greater omentum is a large peritoneal fold consisting of connective tissue, fat and lymphatics. It is well vascularized with large feeding arteries and draining veins. Because harvesting requires laparotomy, this flap is used infrequently. Previous abdominal surgery may render the omentum scarred and adherent to the intra-abdominal contents, and therefore preclude its use.
Vascular Anatomy
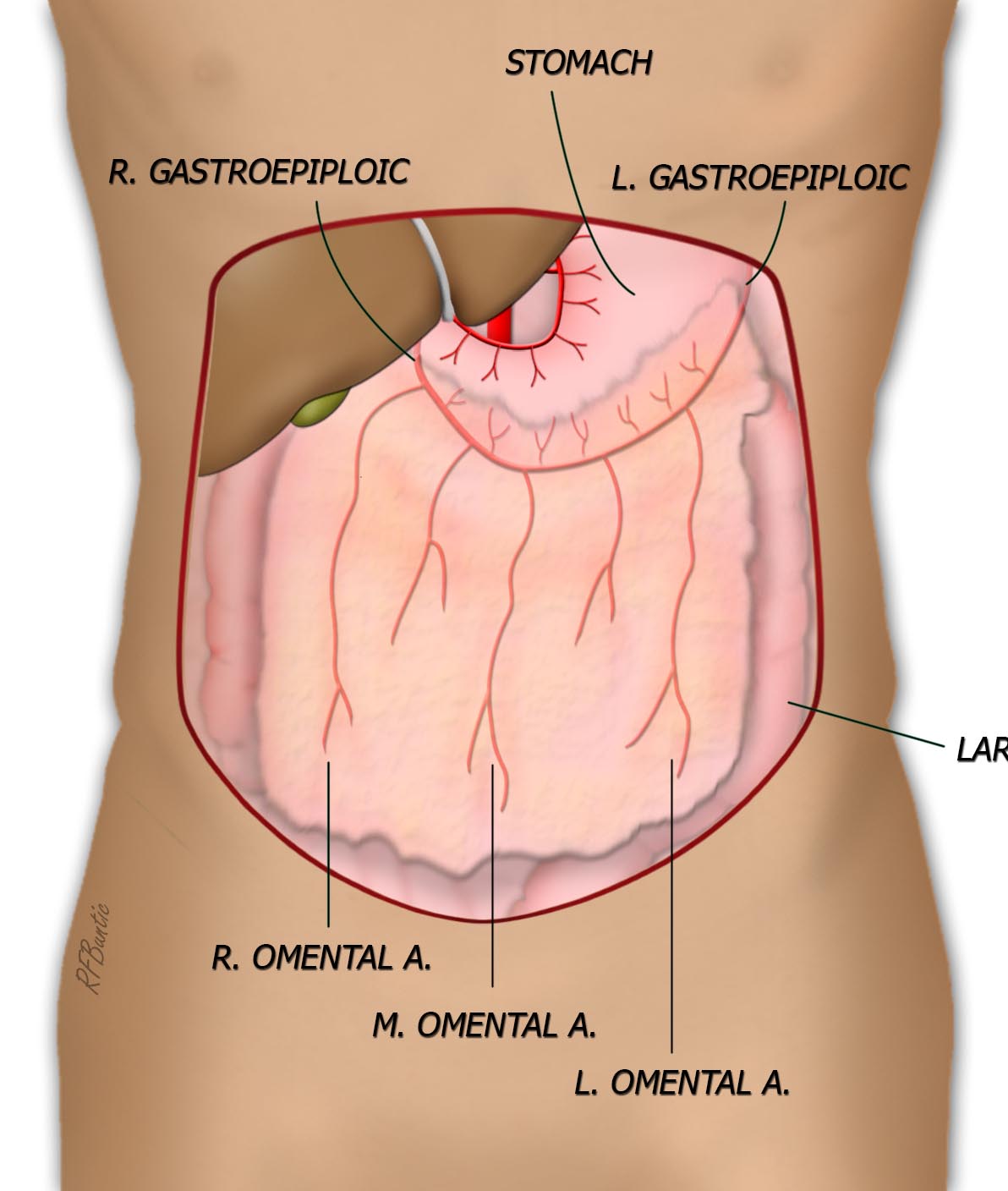
The omentum possesses a rich arterial arcade with three dominant vessels descending from the gastroepiploic artery, along the greater curvature of the stomach. A right, middle and left omental branch arise from gastroepiplic system, with smaller intervening branches and adjacent draining veins. The flap is isolated on the right omental artery and the right gastroepiploic artery.
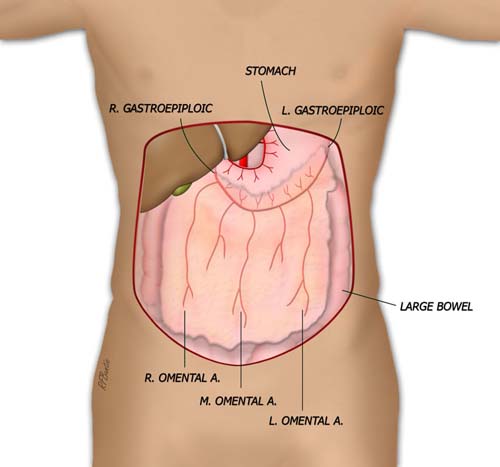
The greater omentum is supplied by three main arterial branches: the right, middle and left omental arteries. These take origin from the gastroepiploics.
Operative Procedure
An upper midline lapartomy incision is used and the omentum is delivered into the operative field. The greater curvature of the stomach and the right and left gastroepiploic vessels are identified as are the major descending branches to the omentum. The omentum is flipped superiorly, exposing the posterior attachements to the large colon. These attachments are freed, with perforating vessels ligated and divided. The omentum is then isolated on its attachment to the greater curvature of the stomach.

The omentum is freed from the posterior attachments on the stomach and the vascular inflow arteries and veins are identified for division. The right omental artery and vein are spared and used for vascular inflow and drainage.
The flap is then dissected free of stomach, beginning on the left side by ligating branches entering the omentum. The left and middle descending branches are divided, as are smaller branches arising from the gastroepiploic system. The entire flap is isolated on the right omental artery pedicle.

The flap is isolated on the pedicle
Post Operative Care
The lapartomy incision necessitates gradual institution of feeding as the small and large bowel begin to resume normal functioning.