The Transverse Upper Gracilis (TUG) Flap
Anatomic considerations
Anatomy
The cutaneous perforators of the gracilis muscle supply both the anterior and posterior inner thigh skin reliably. The transverse orientation of the flap allows for a large skin paddle, with some independence from the muscle below.
The perforator for the transverse upper gracilis flap travels through the gracilis muscle. The muscle is small and expendable, with no resultant hernia formation or bulging after removal.
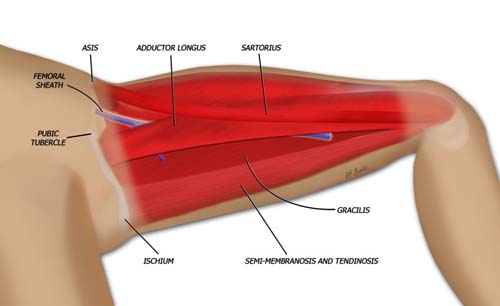
A medial thigh muscle, the gracilis takes origin off the pubic symphysis, inferior pubic ramus and ischium then inserts distally into the medial condyle of the knee. The axis of the muscle can be defined by drawing a line from the ischium to the medial femoral condyle. The axis can be found alternatively by palpating the adductor longus medially with the thigh abducted. The gracilis axis is defined 2 to 3 finger breadths posterior to palpable edge of the adductor longus.

The perforator for the transverse upper gracilis flap travels through the gracilis muscle. The muscle is small and expendable, with no resultant hernia formation or bulging after removal.
The skin paddle of the flap is marked transversely, with the widest point centered over the gracilis muscle. Care must be taken not to resect too much skin, since closure can be difficult.

The flap is harvested from the inner upper thigh, and has a crescent like shape.
The patient is placed in the supine position with the legs abducted and the knees bent. The anterior flap is elevated first.
The flap is elevated superficial to the muscular fascia, preserving or ligating the saphenous vein as necessary for flap harvest.

The flap is marked in the crease of the inner thigh, just below the inguinal ligament and extending posteriorly in the inferior buttock crease.

The anterior flap is elevated, sparing the anterior branch of the saphenous vein. The posterior branch travels within the substance of the flap and is ligated and divided.
When the edge of the adductor longus medial aspect is reached, the muscular fascia is incised and the pedicle to the gracilis is identified under the adductor longus. When the pedicle is identified, the posterior flap can be elevated.

The muscular fascia is incised anterior to the posterior edge of the adductor longus, and the pedicle to the gracilis is identified.
After the posterior flap is elevated, the proximal and distal muscle can be divided. The pedicle is traced to it's origin to gain length as necessary.

Once the pedicle is identified and dissected free the posterior flap is elevated and the proximal and distal ends of the gracilis muscle are divided.
Closure of the would is done in layers over suction drains.